

Current Therapy for Hypoplastic Left Heart Syndrome and Related Single Ventricle Lesions
- PMID: 27777296
- PMCID: PMC5119545
- DOI: 10.1161/CIRCULATIONAHA.116.022816
Current Therapy for Hypoplastic Left Heart Syndrome and Related Single Ventricle Lesions
Abstract
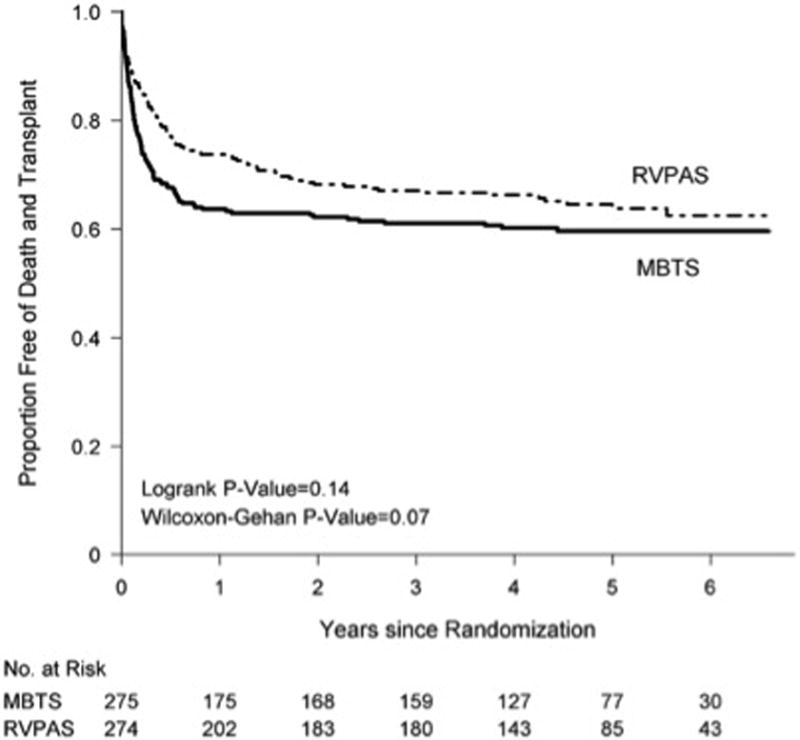
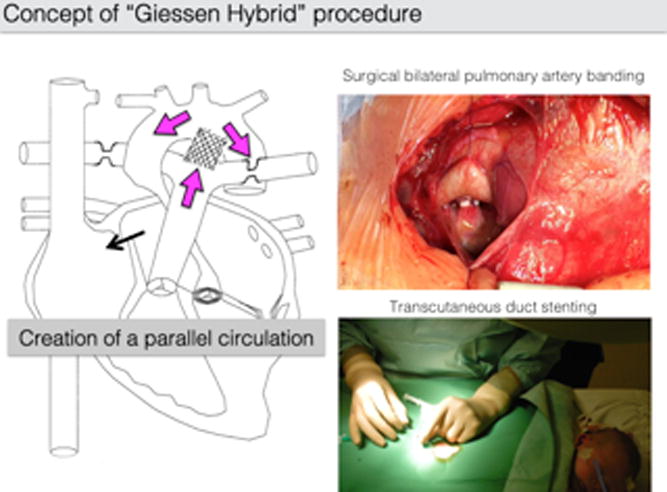
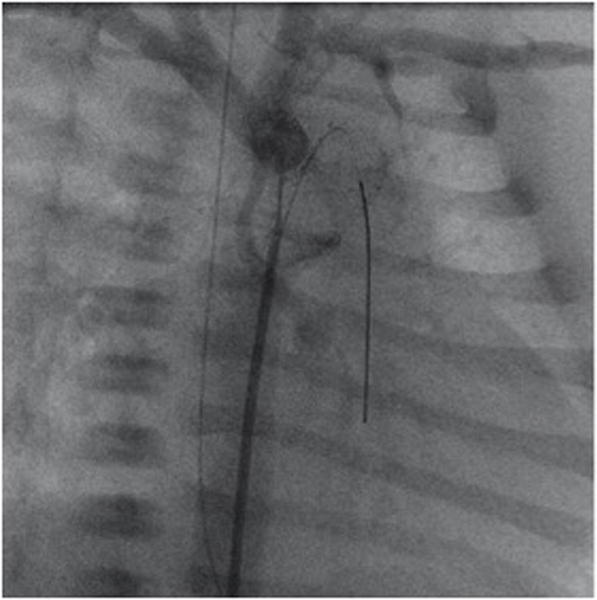
Universally fatal only 4 decades ago, the progress in the 3-stage palliation of hypoplastic left heart syndrome and related single right ventricular lesions has drastically improved the outlook for these patients. Although the stage II operation (hemi-Fontan or bidirectional Glenn) and stage III Fontan procedure have evolved into relatively low-risk operations, the stage I Norwood procedure remains one of the highest-risk and costliest common operations performed in congenital heart surgery. Yet, despite this fact, experienced centers now report hospital survivals of >90% for the Norwood procedure. This traditional 3-stage surgical palliation has seen several innovations in the past decade aimed at improving outcomes, particularly for the Norwood procedure. One significant change is a renewed interest in the right ventricle-to-pulmonary artery shunt as the source of pulmonary blood flow, rather than the modified Blalock-Taussig shunt for the Norwood. The multi-institutional Single Ventricle Reconstruction trial randomly assigned 555 patients to one or the other shunt, and these subjects continue to be followed closely as they now approach 10 years postrandomization. In addition to modifications to the Norwood procedure, the hybrid procedure, a combined catheter-based and surgical approach, avoids the Norwood procedure in the newborn period entirely. The initial hybrid procedure is then followed by a comprehensive stage II, which combines components of both the Norwood and the traditional stage II, and later completion of the Fontan. Proponents of this approach hope to improve not only short-term survival, but also potentially longer-term outcomes, such as neurodevelopment, as well. Regardless of the approach, traditional surgical staged palliation or the hybrid procedure, survivals have vastly improved, and large numbers of these patients are surviving not only through their Fontan in early childhood, but also into adolescence and young adulthood. As this population grows, it becomes increasingly important to understand the longer-term outcomes of these Fontan patients, not only in terms of survival, but also in terms of the burden of disease, neurodevelopmental outcomes, psychosocial development, and quality of life.
Keywords: congenital; heart defects; heart ventricles; hybrid imaging; hypoplastic left heart syndrome; surgery.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Disclosures: None.
Figures
References
-
- Noonan JA, Nadas AS. The hypoplastic left heart syndrome; an analysis of 101 cases. Pediatr Clin North Am. 1958;5:1029–1056. - PubMed
-
- Norwood WI, Lang P, Casteneda AR, Campbell DN. Experience with operations for hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. 1981;82:511–519. - PubMed
-
- Tweddell JS, Hoffman GM, Fedderly RT, Berger S, Thomas JP, Jr, Ghanayem NS, Kessel MW, Litwin SB. Phenoxybenzamine improves systemic oxygen delivery after the Norwood procedure. Ann Thorac Surg. 1999;67:161–167. - PubMed
-
- Norwood WI, Kirklin JK, Sanders SP. Hypoplastic left heart syndrome: experience with palliative surgery. Am J Cardiol. 1980;45:87–91. - PubMed
-
- Ohye RG, Ludomirsky A, Devaney EJ, Bove EL. Comparison of right ventricle to pulmonary artery conduit and modified Blalock–Taussig shunt hemodynamics after the Norwood operation. Ann Thorac Surg. 2004;78:1090–1093. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
