

The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: A systematic review and meta-analysis of randomized and non-randomized studies - The Cardiac Rehabilitation Outcome Study (CROS)
- PMID: 27777324
- PMCID: PMC5119625
- DOI: 10.1177/2047487316671181
The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: A systematic review and meta-analysis of randomized and non-randomized studies - The Cardiac Rehabilitation Outcome Study (CROS)
Abstract
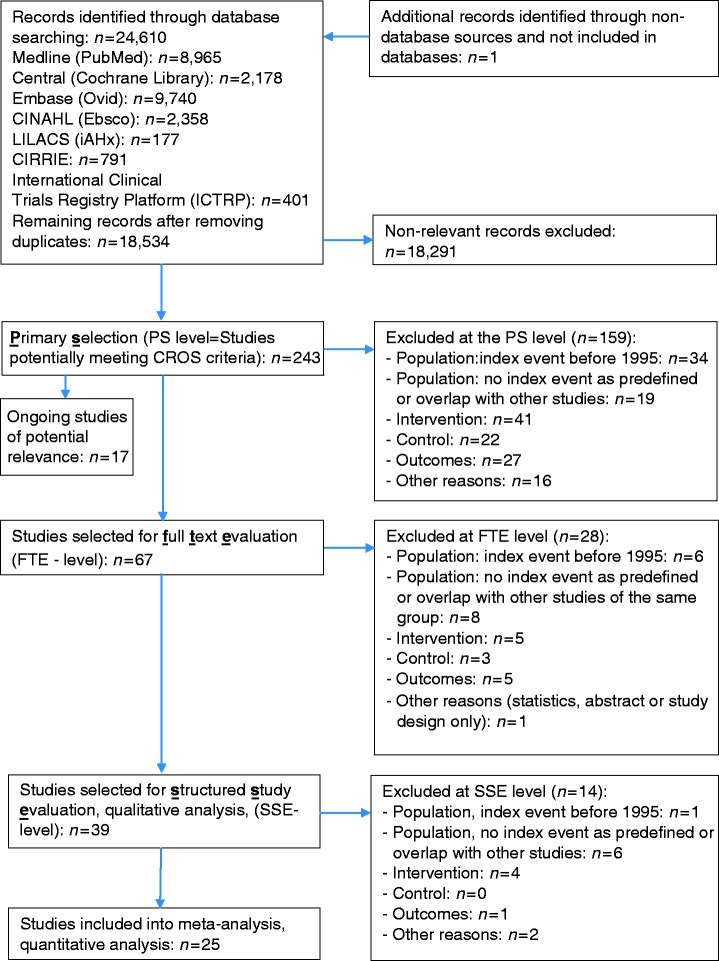
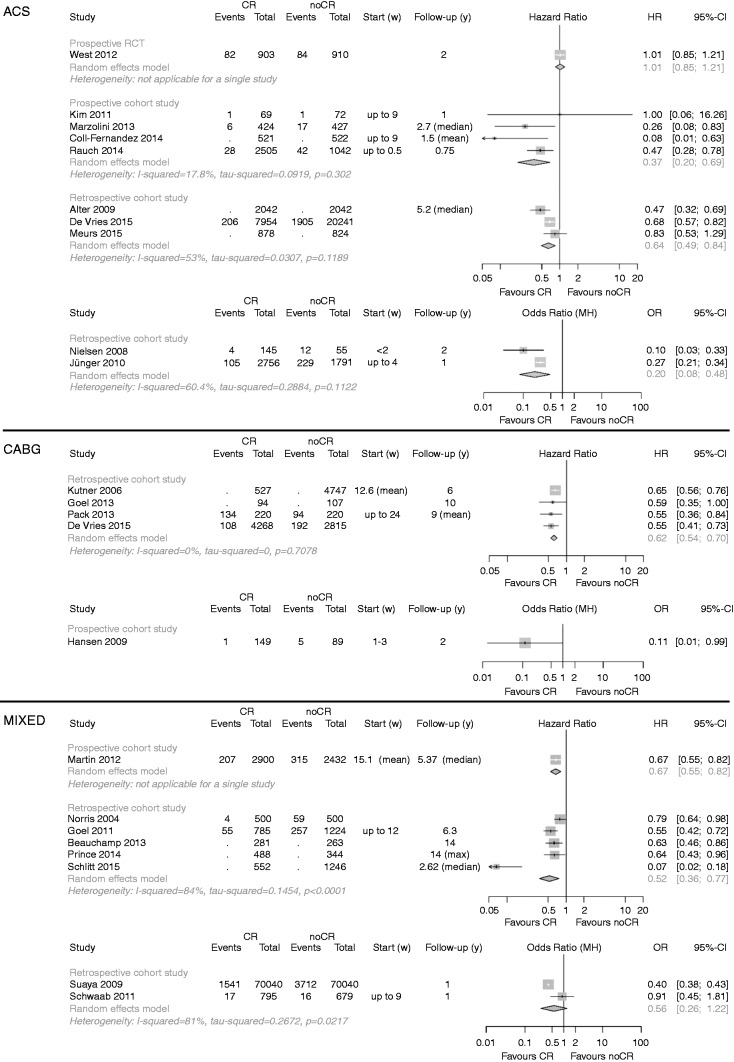
Background The prognostic effect of multi-component cardiac rehabilitation (CR) in the modern era of statins and acute revascularisation remains controversial. Focusing on actual clinical practice, the aim was to evaluate the effect of CR on total mortality and other clinical endpoints after an acute coronary event. Design Structured review and meta-analysis. Methods Randomised controlled trials (RCTs), retrospective controlled cohort studies (rCCSs) and prospective controlled cohort studies (pCCSs) evaluating patients after acute coronary syndrome (ACS), coronary artery bypass grafting (CABG) or mixed populations with coronary artery disease (CAD) were included, provided the index event was in 1995 or later. Results Out of n = 18,534 abstracts, 25 studies were identified for final evaluation (RCT: n = 1; pCCS: n = 7; rCCS: n = 17), including n = 219,702 patients (after ACS: n = 46,338; after CABG: n = 14,583; mixed populations: n = 158,781; mean follow-up: 40 months). Heterogeneity in design, biometrical assessment of results and potential confounders was evident. CCSs evaluating ACS patients showed a significantly reduced mortality for CR participants (pCCS: hazard ratio (HR) 0.37, 95% confidence interval (CI) 0.20-0.69; rCCS: HR 0.64, 95% CI 0.49-0.84; odds ratio 0.20, 95% CI 0.08-0.48), but the single RCT fulfilling Cardiac Rehabilitation Outcome Study (CROS) inclusion criteria showed neutral results. CR participation was also associated with reduced mortality after CABG (rCCS: HR 0.62, 95% CI 0.54-0.70) and in mixed CAD populations. Conclusions CR participation after ACS and CABG is associated with reduced mortality even in the modern era of CAD treatment. However, the heterogeneity of study designs and CR programmes highlights the need for defining internationally accepted standards in CR delivery and scientific evaluation.
Keywords: Rehabilitation; acute coronary syndrome; coronary artery disease; coronary bypass grafting; hospital readmission; mortality.
Figures
Comment in
-
CROS editorial comment: Cardiac rehabilitation effectiveness in the 'new era': Any doubts after an acute coronary event?Eur J Prev Cardiol. 2017 May;24(8):796-798. doi: 10.1177/2047487317694468. Epub 2017 Jan 1. Eur J Prev Cardiol. 2017. PMID: 28436721 No abstract available.
References
-
- Anderson L, Oldridge N, Thompson DR, et al. Exercise-based cardiac rehabilitation for coronary heart disease. J Am Coll Cardiol 2016; 67(1): 1–12. - PubMed
-
- Goel K, Lennon RJ, Tilbury RT, et al. Impact of cardiac rehabilitation on mortality and cardiovascular events after percutaneous coronary intervention in the community. Circulation 2011; 123(21): 2344–2352. - PubMed
-
- Goel K, Pack QR, Lahr B, et al. Cardiac rehabilitation is associated with reduced long-term mortality in patients undergoing combined heart valve and CABG surgery. Eur J Prev Cardiol 2015; 22(2): 159–168. - PubMed
-
- Suaya JA, Stason WB, Ades PA, et al. Cardiac rehabilitation and survival in older coronary patients. J Am Coll Cardiol 2009; 54(1): 25–33. - PubMed
-
- Norris CM, Jensen LA, Galbraith PD, et al. Referral rate and outcomes of cardiac rehabilitation after cardiac catheterization in a large Canadian city. J Cardiopulm Rehabil 2004; 24: 392–400. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
