

Systemic Lupus Erythematosus Presenting as Refractory Thrombotic Thrombocytopenic Purpura: A Diagnostic and Management Challenge. A Case Report and Concise Review of the Literature
- PMID: 27777394
- PMCID: PMC5083062
- DOI: 10.12659/ajcr.898955
Systemic Lupus Erythematosus Presenting as Refractory Thrombotic Thrombocytopenic Purpura: A Diagnostic and Management Challenge. A Case Report and Concise Review of the Literature
Abstract
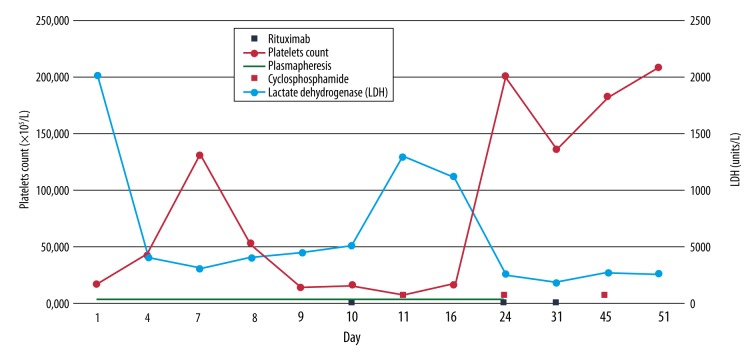
BACKGROUND Thrombotic thrombocytopenic purpura (TTP) is one of the thrombotic microangiopathic (TMA) syndromes, caused by severely reduced activity of the vWF-cleaving protease ADAMTS13. Systemic lupus erythematosus (SLE), on the other hand, is an autoimmune disease that affects various organs in the body, including the hematopoietic system. SLE can present with TMA, and differentiating between SLE and TTP in those cases can be very challenging, particularly in patients with no prior history of SLE. Furthermore, an association between these 2 diseases has been described in the literature, with most of the TTP cases occurring after the diagnosis of SLE. In rare cases, TTP may precede the diagnosis of SLE or occur concurrently. CASE REPORT We present a case of a previously healthy 34-year-old female who presented with dizziness and flu-like symptoms and was found to have thrombocytopenia, hemolytic anemia, and schistocytes in the peripheral smear. She was subsequently diagnosed with TTP and started on plasmapheresis and high-dose steroids, but without a sustained response. A diagnosis of refractory TTP was made, and she was transferred to our facility for further management. Initially, the patient was started on rituximab, but her condition continued to deteriorate, with worsening thrombocytopenia. Later, she also fulfilled the Systemic Lupus International Collaborating Clinics (SLICC) criteria for diagnosis of SLE. Treatment of TTP in SLE patients is generally similar to that in the general population, but in refractory cases there are few reports in the literature that show the efficacy of cyclophosphamide. We started our patient on cyclophosphamide and noticed a sustained improvement in the platelet count in the following weeks. CONCLUSIONS Thrombotic thrombocytopenic purpura is a life-threatening hematological emergency which must be diagnosed and treated in a timely manner. Refractory cases of TTP have been described in the literature, but without clear evidence-based guidelines for its management, and is solely based on expert opinion and previous case reports. Further studies are needed to establish guidelines for its management. We present this case to highlight the role that cyclophosphamide might carry in those cases and to be a foundation for these future studies.
Conflict of interest statement
Conflicts of Interest: None declared
Figures
References
-
- George JN, Nester CM. Syndromes of thrombotic microangiopathy. N Engl J Med. 2014;371(7):654–66. - PubMed
-
- Nesher G, Hanna VE, Moore TL, et al. Thrombotic microangiographic hemolytic anemia in systemic lupus erythematosus. Semin Arthritis Rheum. 1994;24(3):165–72. - PubMed
-
- Musio F, Bohen EM, Yuan CM, Welch PG. Review of thrombotic thrombocytopenic purpura in the setting of systemic lupus erythematosus. Semin Arthritis Rheum. 1998;28(1):1–19. - PubMed
-
- Matsuyama T, Kuwana M, Matsumoto M, et al. Heterogeneous pathogenic processes of thrombotic microangiopathies in patients with connective tissue diseases. Thromb Haemost. 2009;102(2):371–78. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
