

Abdominal vascular syndromes: characteristic imaging findings
- PMID: 27777480
- PMCID: PMC5073393
- DOI: 10.1590/0100-3984.2015.0136
Abdominal vascular syndromes: characteristic imaging findings
Abstract
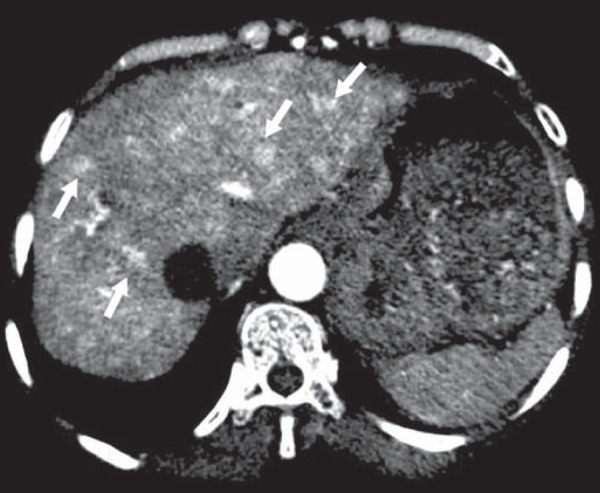
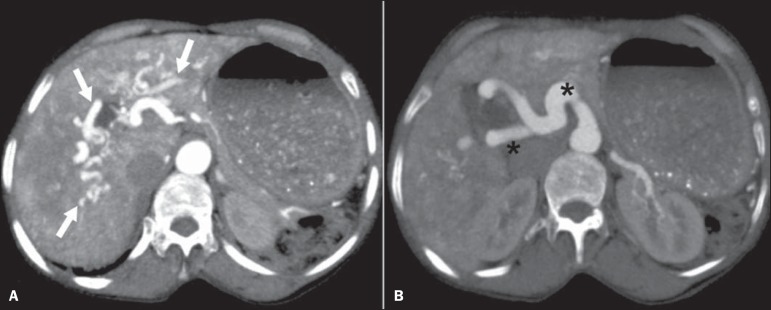
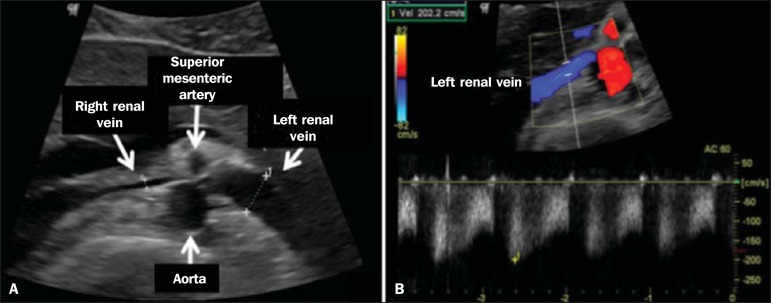
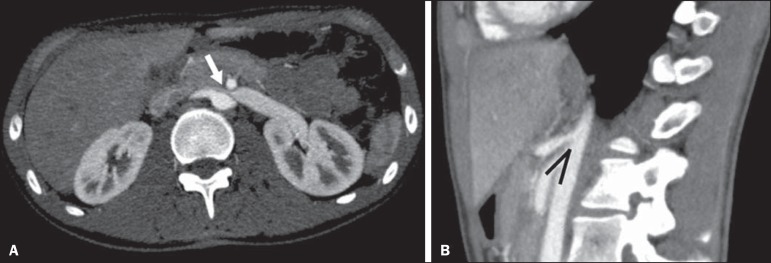
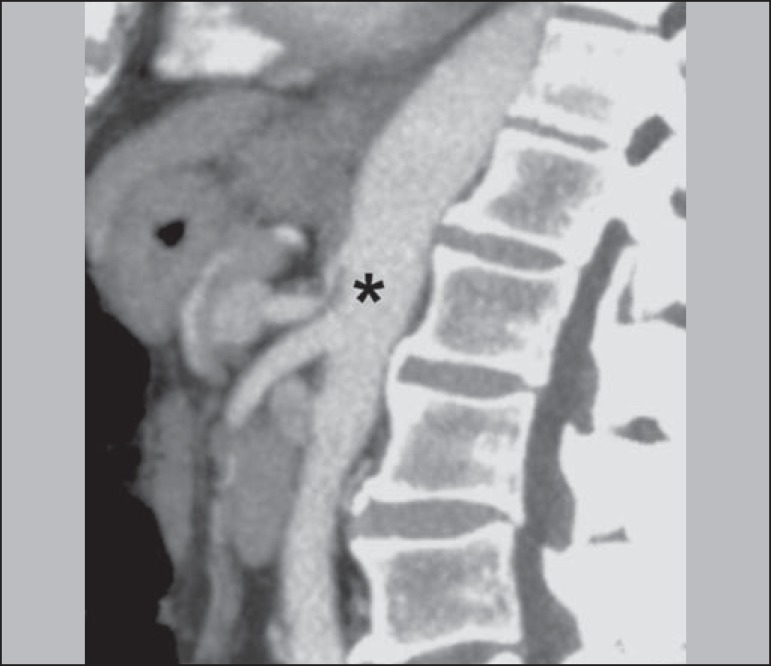
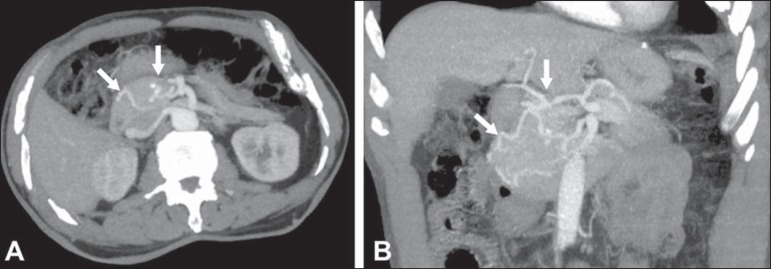
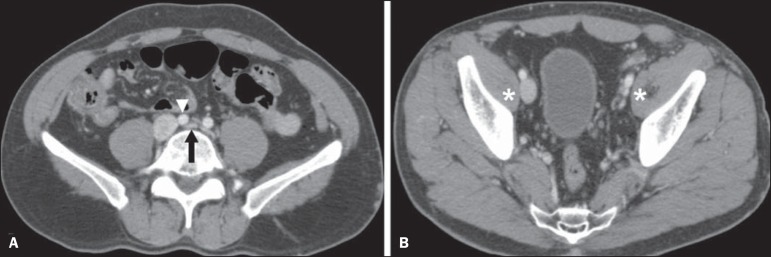
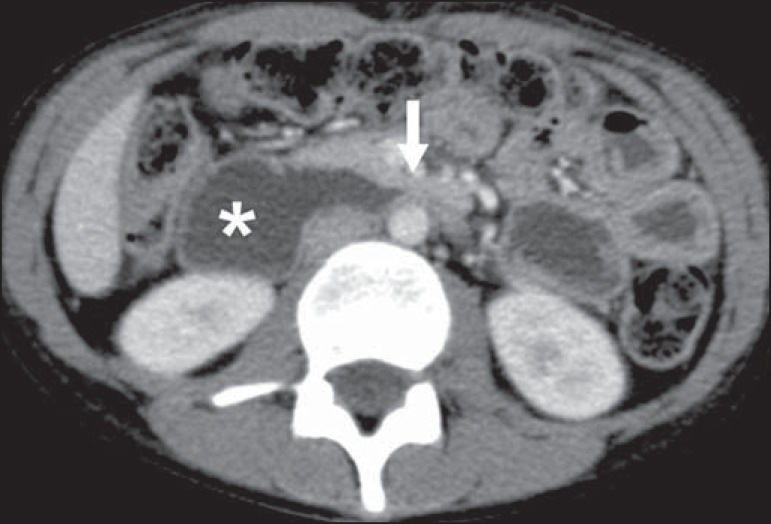
Abdominal vascular syndromes are rare diseases. Although such syndromes vary widely in terms of symptoms and etiologies, certain imaging findings are characteristic. Depending on their etiology, they can be categorized as congenital-including blue rubber bleb nevus syndrome, Klippel-Trenaunay syndrome, and hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome)-or compressive-including "nutcracker" syndrome, median arcuate ligament syndrome, Cockett syndrome (also known as May-Thurner syndrome), and superior mesenteric artery syndrome. In this article, we aimed to illustrate imaging findings that are characteristic of these syndromes, through studies conducted at our institution, as well as to perform a brief review of the literature on this topic.
As síndromes vasculares abdominais englobam doenças raras, com sintomas e causas diversas, mas com achados de imagem característicos. Dividem-se em dois grupos distintos, a depender de sua origem, que pode ser congênita (síndrome de blue rubber bleb nevus, síndrome de Klippel-Trenaunay e telangiectasia hereditária hemorrágica/Rendu-Osler-Weber) ou compressiva (síndrome do "quebra-nozes", síndrome do ligamento arqueado, síndrome de Cockett ou May-Thurner e síndrome da artéria mesentérica superior). Neste artigo, o nosso objetivo é ilustrar achados de imagens determinantes dessas doenças, por meio de estudos adquiridos em nossa instituição, associando uma breve revisão da literatura.
Keywords: Arteriovenous fistula; Fístula arteriovenosa; Gastrointestinal tract; Hemangioma; Trato gastrintestinal; Trombose venosa; Venous thrombosis.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources