

Phenotypic and Functional Dysregulated Blood NK Cells in Colorectal Cancer Patients Can Be Activated by Cetuximab Plus IL-2 or IL-15
- PMID: 27777574
- PMCID: PMC5056190
- DOI: 10.3389/fimmu.2016.00413
Phenotypic and Functional Dysregulated Blood NK Cells in Colorectal Cancer Patients Can Be Activated by Cetuximab Plus IL-2 or IL-15
Abstract
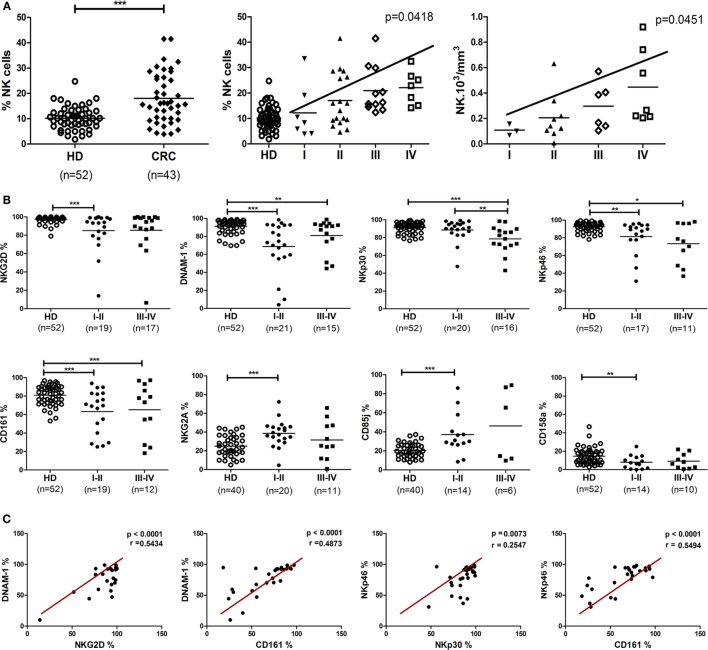
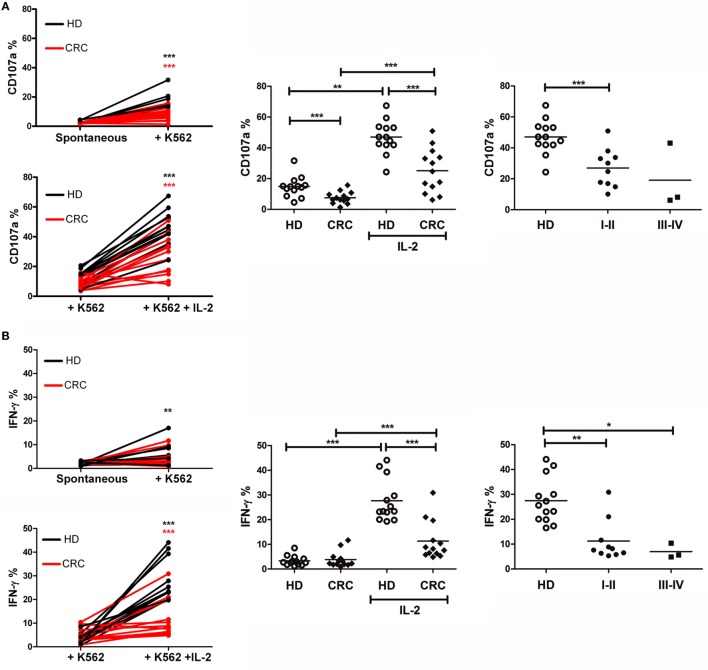
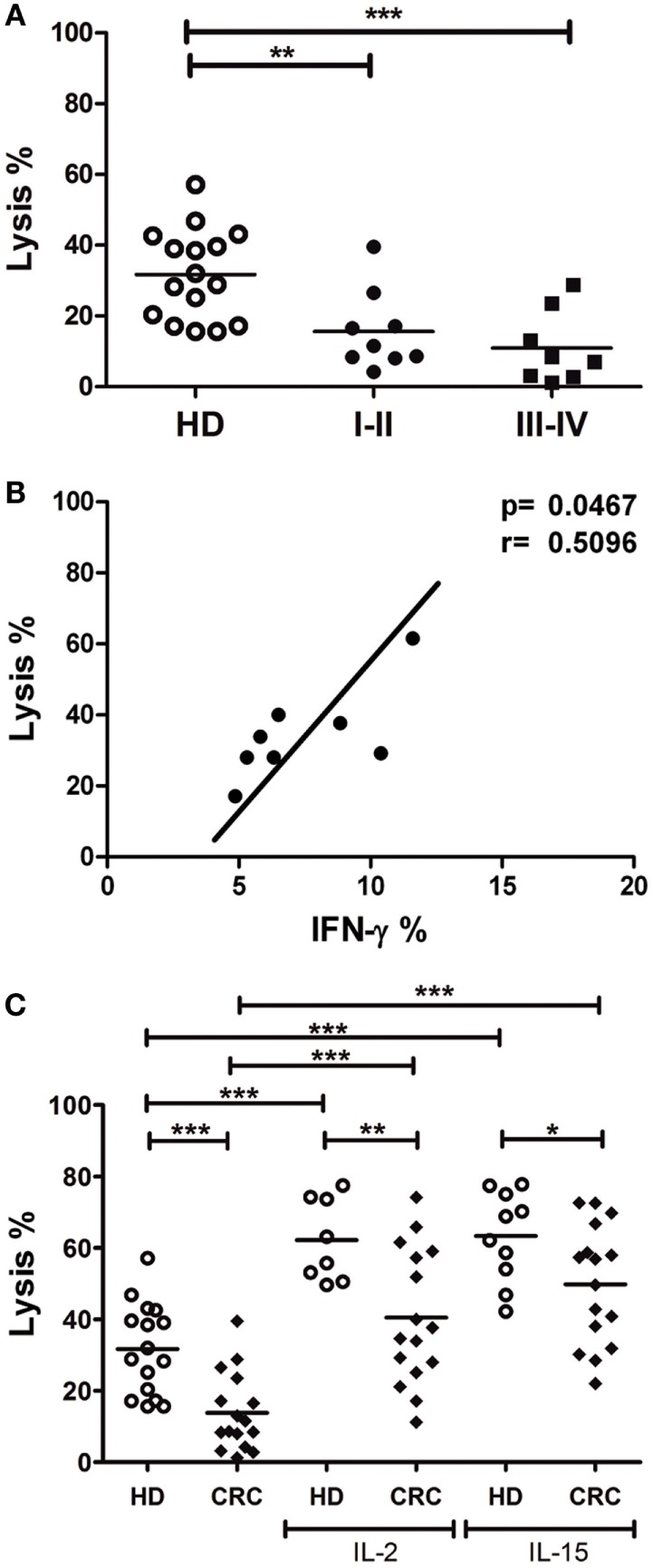
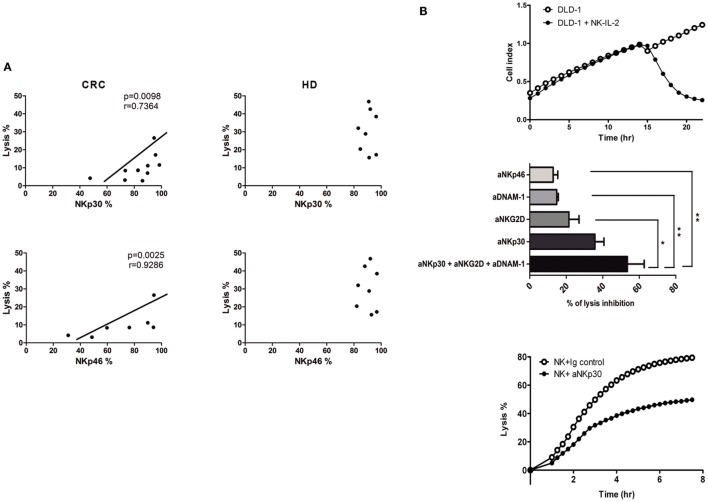
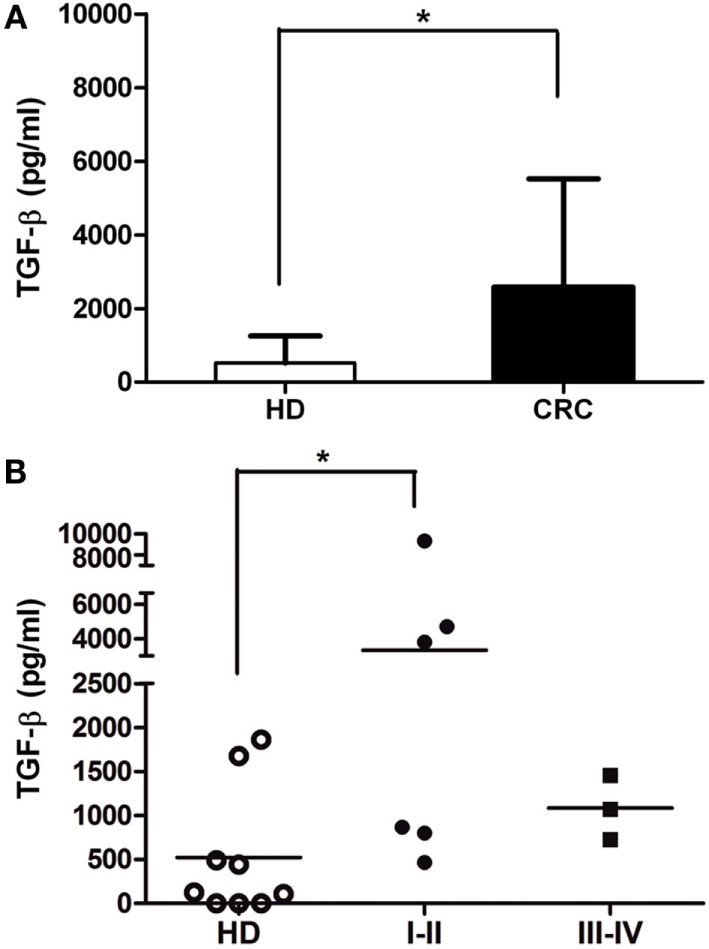
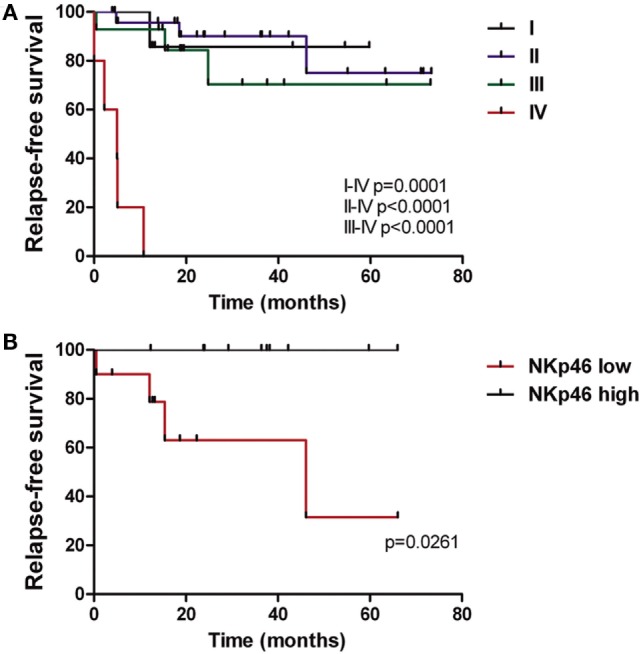
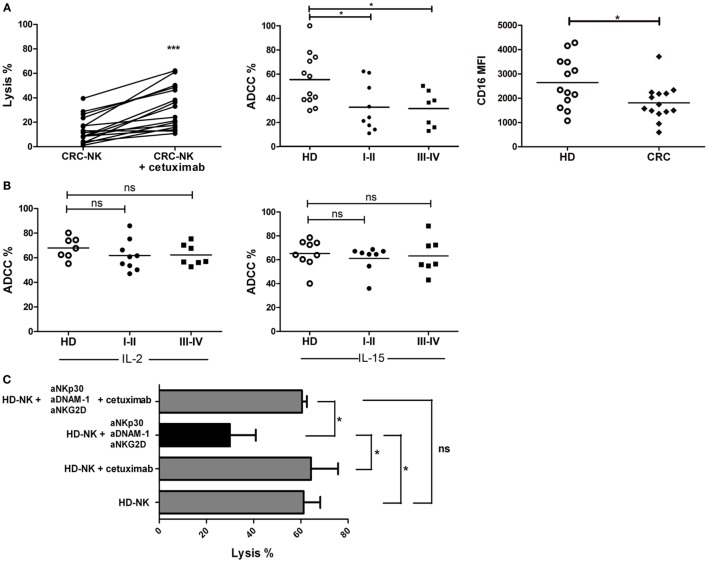
The clinical outcome of colorectal cancer (CRC) is associated with the immune response; thus, these tumors could be responsive to different immune therapy approaches. Natural killer (NK) cells are key antitumor primary effectors that can eliminate CRC cells without prior immunization. We previously determined that NK cells from the local tumor environment of CRC tumors display a profoundly altered phenotype compared with circulating NK cells from healthy donors (HD). In this study, we evaluated peripheral blood NK cells from untreated patients and their possible role in metastasis progression. We observed profound deregulation in receptor expression even in early stages of disease compared with HD. CRC-NK cells displayed underexpression of CD16, NKG2D, DNAM-1, CD161, NKp46, and NKp30 activating receptors, while inhibitory receptors CD85j and NKG2A were overexpressed. This inhibited phenotype affected cytotoxic functionality against CRC cells and interferon-γ production. We also determined that NKp30 and NKp46 are the key receptors involved in detriment of CRC-NK cells' antitumor activity. Moreover, NKp46 expression correlated with relapse-free survival of CRC patients with a maximum follow-up of 71 months. CRC-NK cells also exhibited altered antibody-dependent cellular cytotoxicity function responding poorly to cetuximab. IL-2 and IL-15 in combination with cetuximab stimulated NK cell, improving cytotoxicity. These results show potential strategies to enhance CRC-NK cell activity.
Keywords: IL-15; IL-2; NKp30; NKp46; cetuximab; colorectal cancer; natural killer cells.
Figures
References
-
- Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med (2006) 355(24):2542–50. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources