

The Etiology and Pathogenesis of Kienböck Disease
- PMID: 27777813
- PMCID: PMC5074830
- DOI: 10.1055/s-0036-1583755
The Etiology and Pathogenesis of Kienböck Disease
Erratum in
-
Erratum: The Etiology and Pathogenesis of Kienböck Disease.J Wrist Surg. 2016 Nov;5(4):e1. doi: 10.1055/s-0036-1584237. Epub 2016 May 18. J Wrist Surg. 2016. PMID: 27779256 Free PMC article.
Abstract
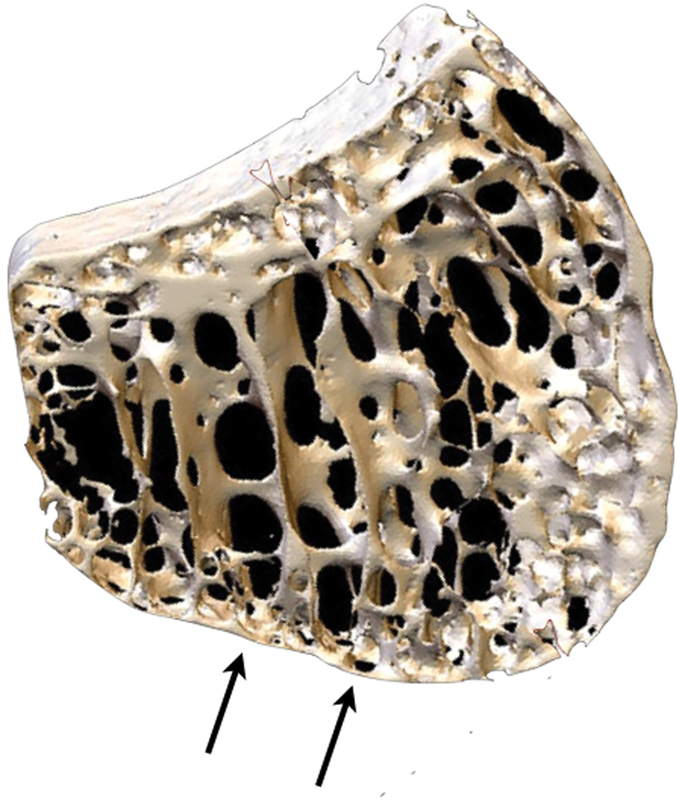
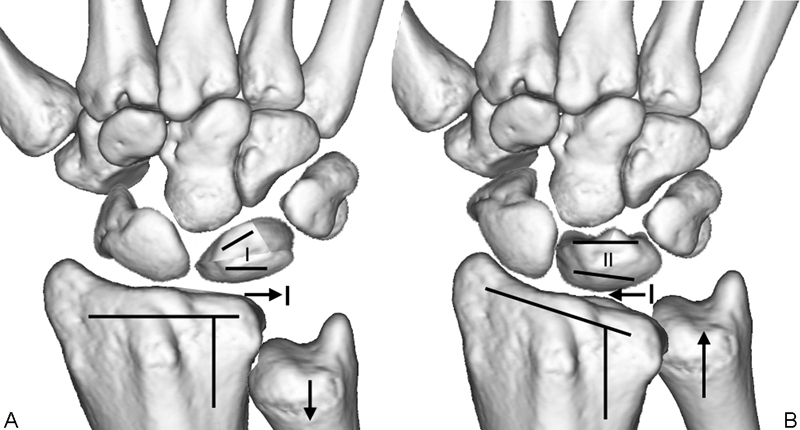
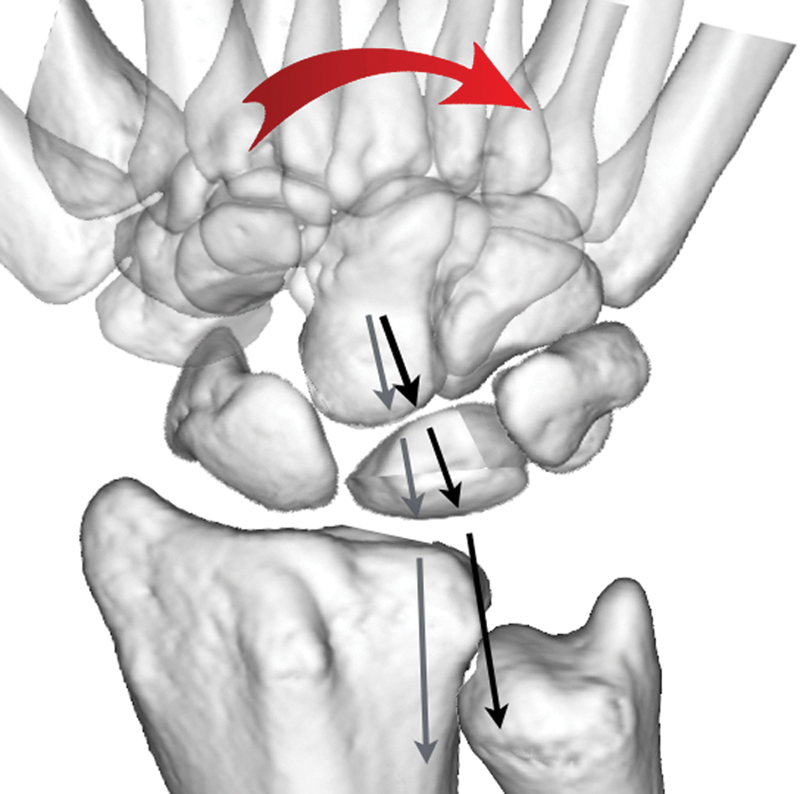
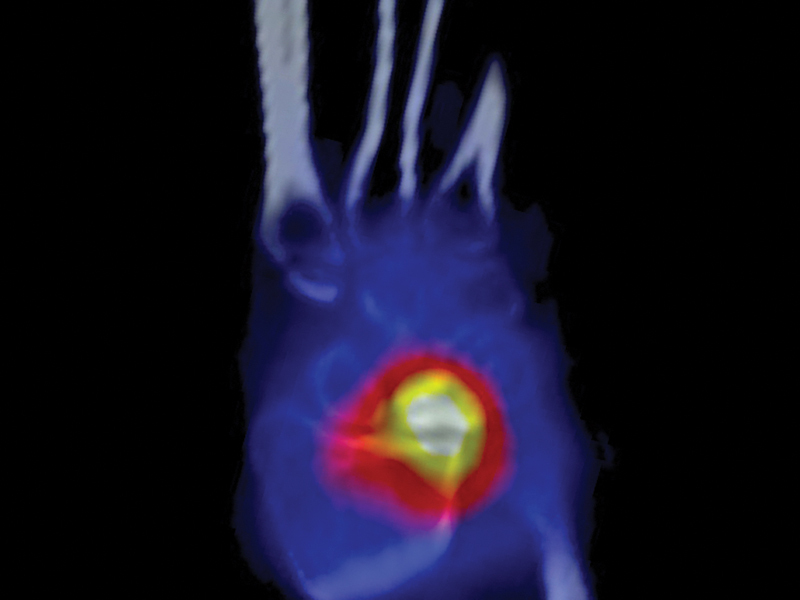
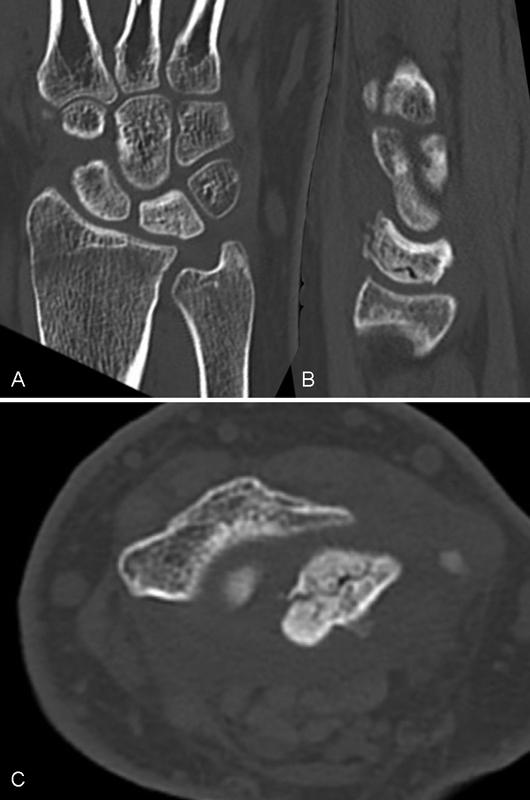
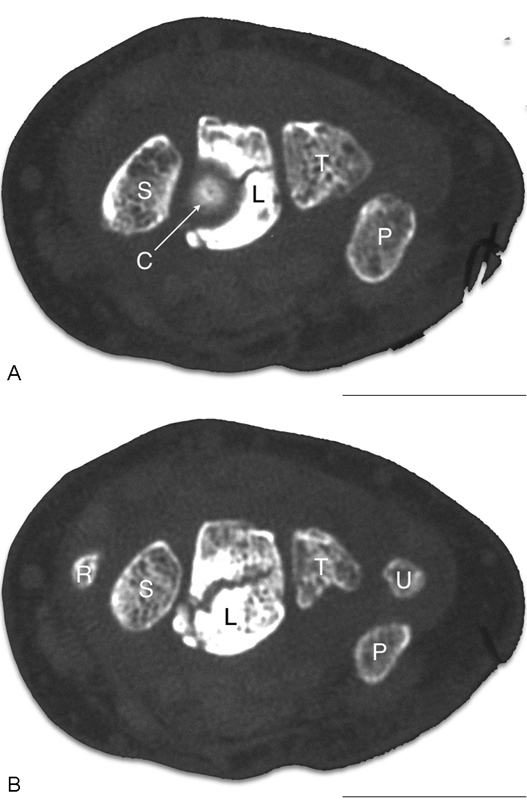
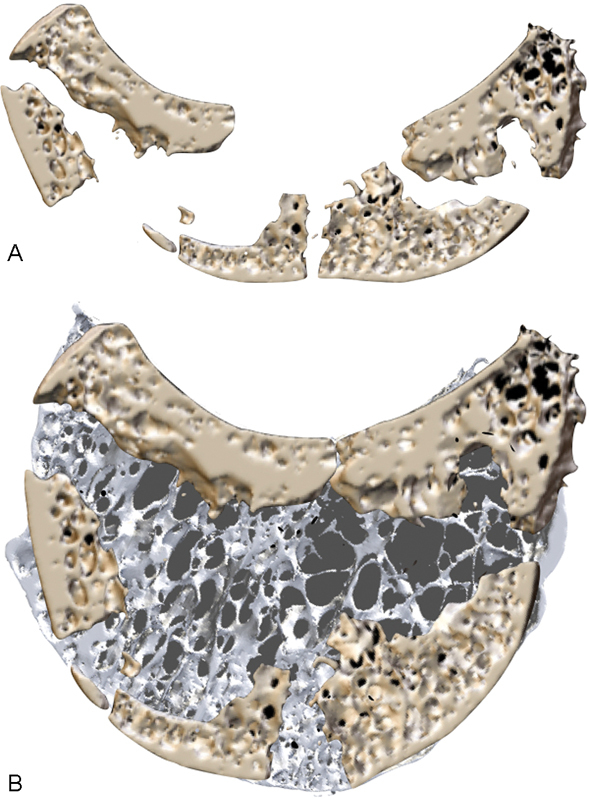
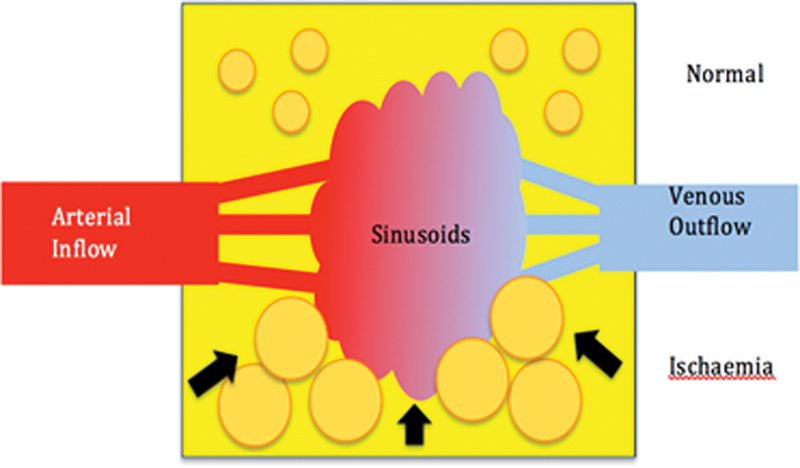
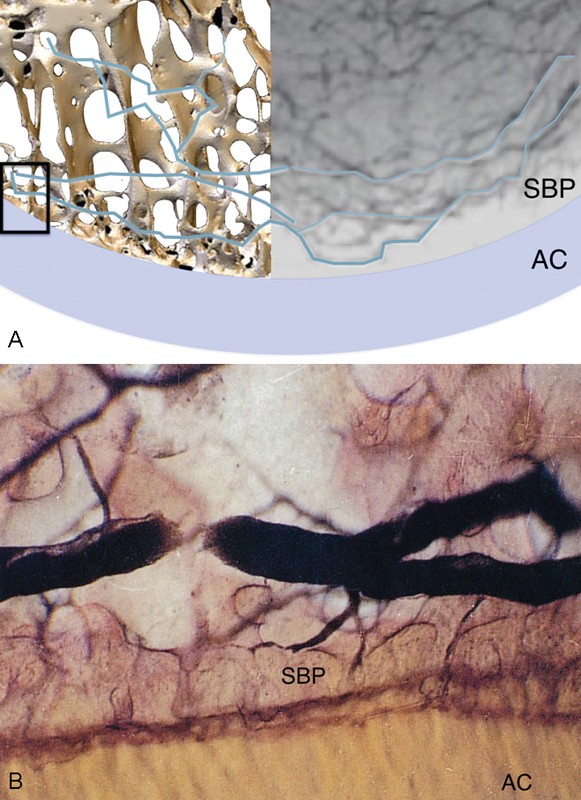
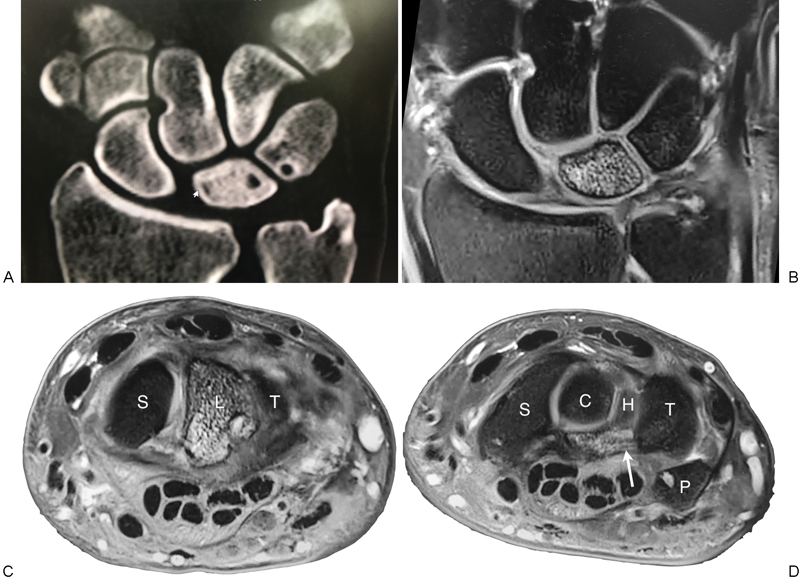
Kienböck disease is a condition that typically occurs in the "at-risk" patient, in the "at-risk" aspect of the proximal condyle of the "at-risk" lunate. In the active male, repetitive loading causes the stress fracture that commences in the single layer proximal subchondral bone plate. The lunate fracture commences at the point the lunate cantilevers over the edge of the distal radius, and then takes on the shape of the radius. We postulate that the stress fracture violates the parallel veins of the venous subarticular plexus-leading to localized venous hypertension and subsequent ischemia and edema of the fatty marrow. The increased osseous compartment pressure further potentiates the venous obstruction, producing avascular necrosis. If the fracture remains localized, it can heal or settle into a stable configuration, so that the wrist remains functional. Fractures of the subchondral bone plate produce irregularity of the lunate articular surfaces and secondary "kissing lesions" of the lunate facet and capitate, and subsequent degeneration. The lunate collapses when the fracture is comminuted, or there is disruption of the spanning trabeculae or a coronal fracture. The secondary effect of the lunate collapse is proximal migration of the capitate between the volar and dorsal fragments, producing collapse of the entire central column. The proximal carpal row is now unstable, and is similar to scapholunate instability, where the capitate migrates between the scaphoid and lunate. The scaphoid is forced into flexion by the trapezium, however, degeneration of the scaphoid and scaphoid facet only occurs in late disease or following failed surgery. In Kienböck disease, the secondary effects of the collapsing lunate are a "compromised" wrist, including: deformity and collapse of the central column, degeneration of the central column (perilunate) articulations, proximal row instability (i.e., between the central and radial columns), and degeneration of the radial column.
Keywords: Kienböck disease; etiology; lunate; pathogenesis.
Conflict of interest statement
Figures
References
-
- Kienböck R. Concerning traumatic malacia of the lunate and its consequences: joint degeneration and compression. Fortsch Geb Roentgen. 1910;16:77–103. - PubMed
-
- Müller W. Über die Erweichung und Verdichtung des Os lunatum, eine typische Erkrankung des Handgelenks. Beitr Klin Chir. 1920;119:664.
-
- Ringsted A. Kienböck bei 2 Br ü dern. Acta Chir Scand. 1932;xx:185–196.
-
- Templeman D, Engber W. Kienbock's Disease—Case Report of Familial Occurrence. Iowa Orthop J. 1985;5:107–109.
-
- Gelberman R H, Bauman T D, Menon J, Akeson W H. The vascularity of the lunate bone and Kienböck's disease. J Hand Surg Am. 1980;5(3):272–278. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
