

Current management of aneurysmal bone cysts
- PMID: 27778155
- PMCID: PMC5127951
- DOI: 10.1007/s12178-016-9371-6
Current management of aneurysmal bone cysts
Abstract
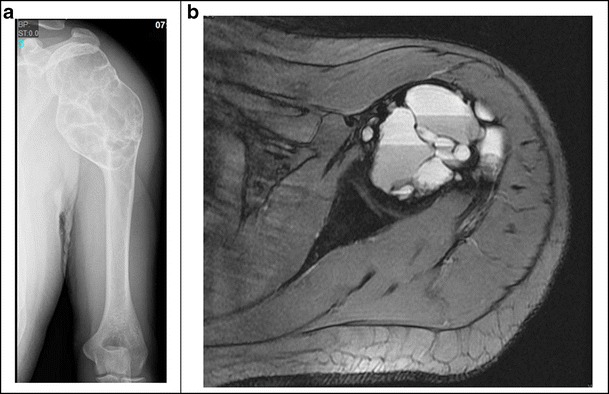
Aneurysmal bone cysts (ABCs) are benign bone lesions arising predominantly in the pediatric population that can cause local pain, swelling, and pathologic fracture. Primary lesions, which constitute roughly two thirds of all ABCs, are thought to be neoplastic in nature, with one third of ABCs arising secondary to other tumors. Diagnosis is made with various imaging modalities, which exhibit characteristic features such as "fluid-fluid levels," although biopsy is critical, as telangiectatic osteosarcoma cannot be excluded based on imaging alone. Currently, the standard of care and most widely employed treatment is intralesional curettage. However, tumor recurrence with curettage alone is common and has driven some to propose a multitude of adjuvants with varying efficacy and risk profiles. Historically, therapies such as en bloc resection or radiation therapy were utilized as an alternative to decrease the recurrence rate, but these therapies imposed high morbidity. As a result, modern techniques now seek to simultaneously reduce morbidity and recurrence, the pursuit of which has produced preliminary study into minimally invasive percutaneous treatments and medical management.
Keywords: Aneurysmal bone cyst; Benign bone tumor; Pediatric tumor.
Conflict of interest statement
Howard Y. Park, Sara K. Yang, William L. Sheppard, Vishal Hegde, Stephen D. Zoller, Scott D. Nelson, and Noah Federman declare that they have no conflict of interest. Nicholas M Bernthal reports personal fees from Onkos and grants from NIH, OREF, POSNA, and MTF outside of the submitted work. Human and animal rights and informed consent This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures



References
-
- JAFFE HL. Solitary unicameral bone cyst. Arch Surg. 1942;44(6):1004. doi: 10.1001/archsurg.1942.01210240043003. - DOI
-
- Fletcher CDM, Unni KK, Mertens F. World Health Organization classification of tumours. Lyon: IARC Press; 2002. Pathology and genetics of tumours of soft tissue and bone.
-
- Leithner A, Windhager R, Lang S, Haas OA, Kainberger F, Kotz R. Aneurysmal bone cyst. A population based epidemiologic study and literature review. Clin Orthop Relat Res. 1999;(363):176–9. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10379320. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
