

Survival Benefit of Lung Transplantation in the Modern Era of Lung Allocation
- PMID: 27779905
- PMCID: PMC5427730
- DOI: 10.1513/AnnalsATS.201606-507OC
Survival Benefit of Lung Transplantation in the Modern Era of Lung Allocation
Abstract
Rationale: Lung transplantation is an accepted and increasingly employed treatment for advanced lung diseases, but the anticipated survival benefit of lung transplantation is poorly understood.
Objectives: To determine whether and for which patients lung transplantation confers a survival benefit in the modern era of U.S. lung allocation.
Methods: Data on 13,040 adults listed for lung transplantation between May 2005 and September 2011 were obtained from the United Network for Organ Sharing. A structural nested accelerated failure time model was used to model the survival benefit of lung transplantation over time. The effects of patient, donor, and transplant center characteristics on the relative survival benefit of transplantation were examined.
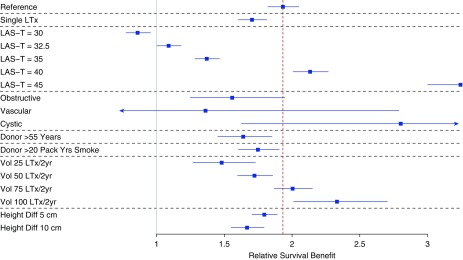
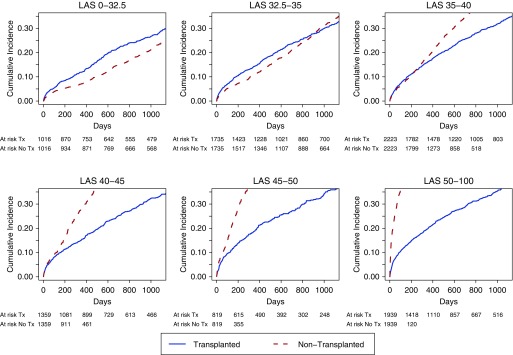
Measurements and main results: Overall, 73.8% of transplant recipients were predicted to achieve a 2-year survival benefit with lung transplantation. The survival benefit of transplantation varied by native disease group (P = 0.062), with 2-year expected benefit in 39.2 and 98.9% of transplants occurring in those with obstructive lung disease and cystic fibrosis, respectively, and by lung allocation score at the time of transplantation (P < 0.001), with net 2-year benefit in only 6.8% of transplants occurring for lung allocation score less than 32.5 and in 99.9% of transplants for lung allocation score exceeding 40.
Conclusions: A majority of adults undergoing transplantation experience a survival benefit, with the greatest potential benefit in those with higher lung allocation scores or restrictive native lung disease or cystic fibrosis. These results provide novel information to assess the expected benefit of lung transplantation at an individual level and to enhance lung allocation policy.
Keywords: lung allocation score; lung transplantation; structural nested accelerated failure time model; survival benefit.
Figures
Comment in
-
Estimating the Survival Benefit of Lung Transplantation: Considering the Disease Course during the Wait.Ann Am Thorac Soc. 2017 Feb;14(2):163-164. doi: 10.1513/AnnalsATS.201611-853ED. Ann Am Thorac Soc. 2017. PMID: 28146388 No abstract available.
-
Improving Donor Lung Management and Recipient Selection in Lung Transplantation.Am J Respir Crit Care Med. 2017 Sep 15;196(6):782-784. doi: 10.1164/rccm.201703-0662RR. Am J Respir Crit Care Med. 2017. PMID: 28608711 No abstract available.
References
-
- Kotloff RM, Thabut G. Lung transplantation. Am J Respir Crit Care Med. 2011;184:159–171. - PubMed
-
- Yusen RD, Edwards LB, Kucheryavaya AY, Benden C, Dipchand AI, Goldfarb SB, Levvey BJ, Lund LH, Meiser B, Rossano JW, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-Second Official Adult Lung and Heart–Lung Transplantation Report—2015; focus theme: early graft failure. J Heart Lung Transplant. 2015;34:1264–1277. - PubMed
-
- Yusen RD, Christie JD, Edwards LB, Kucheryavaya AY, Benden C, Dipchand AI, Dobbels F, Kirk R, Lund LH, Rahmel AO, et al. International Society for Heart and Lung Transplantation. The Registry of the International Society for Heart and Lung Transplantation: Thirtieth Adult Lung and Heart–Lung Transplant Report—2013; focus theme: age. J Heart Lung Transplant. 2013;32:965–978. - PubMed
-
- Charman SC, Sharples LD, McNeil KD, Wallwork J. Assessment of survival benefit after lung transplantation by patient diagnosis. J Heart Lung Transplant. 2002;21:226–232. - PubMed
-
- De Meester J, Smits JM, Persijn GG, Haverich A. Listing for lung transplantation: life expectancy and transplant effect, stratified by type of end-stage lung disease, the Eurotransplant experience. J Heart Lung Transplant. 2001;20:518–524. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
