

The Global Burden of Latent Tuberculosis Infection: A Re-estimation Using Mathematical Modelling
- PMID: 27780211
- PMCID: PMC5079585
- DOI: 10.1371/journal.pmed.1002152
The Global Burden of Latent Tuberculosis Infection: A Re-estimation Using Mathematical Modelling
Abstract
Background: The existing estimate of the global burden of latent TB infection (LTBI) as "one-third" of the world population is nearly 20 y old. Given the importance of controlling LTBI as part of the End TB Strategy for eliminating TB by 2050, changes in demography and scientific understanding, and progress in TB control, it is important to re-assess the global burden of LTBI.
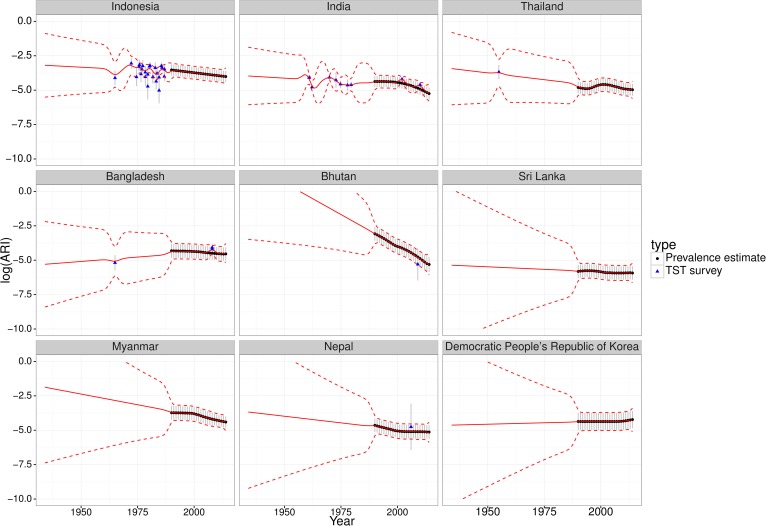
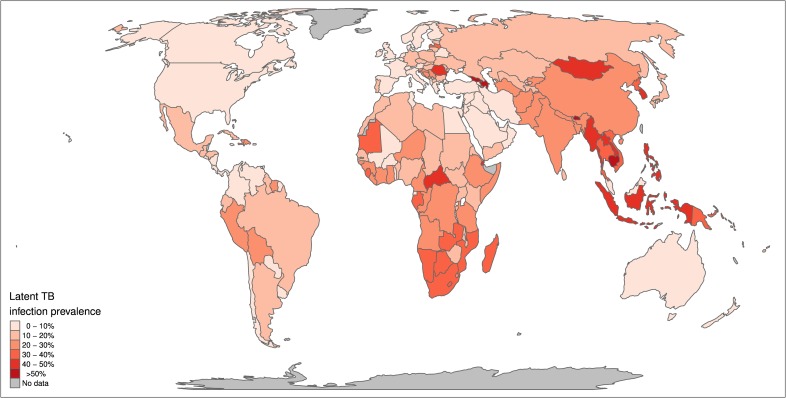
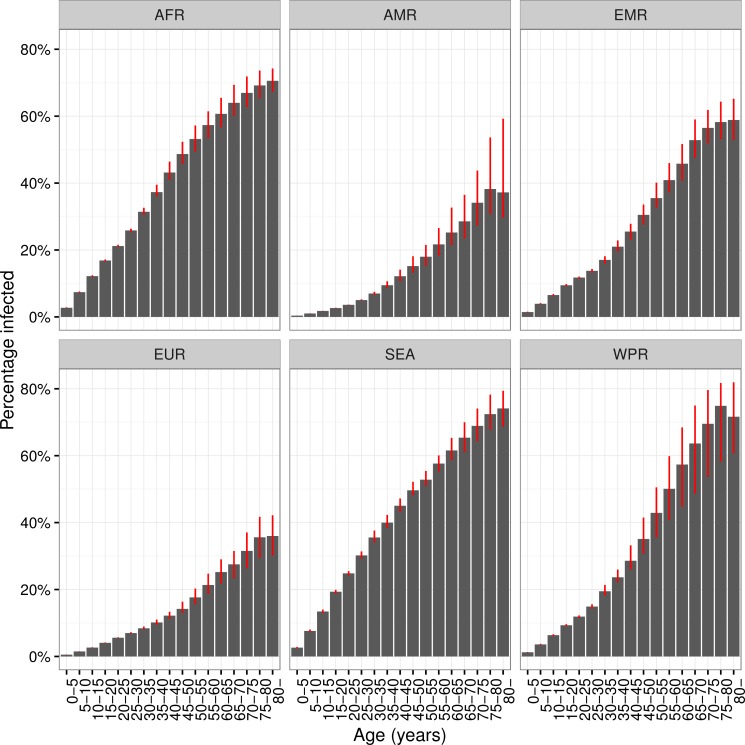
Methods and findings: We constructed trends in annual risk in infection (ARI) for countries between 1934 and 2014 using a combination of direct estimates of ARI from LTBI surveys (131 surveys from 1950 to 2011) and indirect estimates of ARI calculated from World Health Organisation (WHO) estimates of smear positive TB prevalence from 1990 to 2014. Gaussian process regression was used to generate ARIs for country-years without data and to represent uncertainty. Estimated ARI time-series were applied to the demography in each country to calculate the number and proportions of individuals infected, recently infected (infected within 2 y), and recently infected with isoniazid (INH)-resistant strains. Resulting estimates were aggregated by WHO region. We estimated the contribution of existing infections to TB incidence in 2035 and 2050. In 2014, the global burden of LTBI was 23.0% (95% uncertainty interval [UI]: 20.4%-26.4%), amounting to approximately 1.7 billion people. WHO South-East Asia, Western-Pacific, and Africa regions had the highest prevalence and accounted for around 80% of those with LTBI. Prevalence of recent infection was 0.8% (95% UI: 0.7%-0.9%) of the global population, amounting to 55.5 (95% UI: 48.2-63.8) million individuals currently at high risk of TB disease, of which 10.9% (95% UI:10.2%-11.8%) was isoniazid-resistant. Current LTBI alone, assuming no additional infections from 2015 onwards, would be expected to generate TB incidences in the region of 16.5 per 100,000 per year in 2035 and 8.3 per 100,000 per year in 2050. Limitations included the quantity and methodological heterogeneity of direct ARI data, and limited evidence to inform on potential clearance of LTBI.
Conclusions: We estimate that approximately 1.7 billion individuals were latently infected with Mycobacterium tuberculosis (M.tb) globally in 2014, just under a quarter of the global population. Investment in new tools to improve diagnosis and treatment of those with LTBI at risk of progressing to disease is urgently needed to address this latent reservoir if the 2050 target of eliminating TB is to be reached.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organisation. Global Tuberculosis Report 2015. Geneva: 2015. http://www.who.int/tb/publications/global_report/en/ (Accessed 23 September 2016)
-
- Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC. Consensus statement. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA: the journal of the American Medical Association. 1999;282(7):677–86. Epub 1999/10/12. . - PubMed
-
- World Health Organisation. Tuberculosis Fact Sheet 2015 [1st March 2016]. http://www.who.int/mediacentre/factsheets/fs104/en/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
