

Somatostatin receptor based PET/CT in patients with the suspicion of cardiac sarcoidosis: an initial comparison to cardiac MRI
- PMID: 27780922
- PMCID: PMC5363622
- DOI: 10.18632/oncotarget.12799
Somatostatin receptor based PET/CT in patients with the suspicion of cardiac sarcoidosis: an initial comparison to cardiac MRI
Abstract
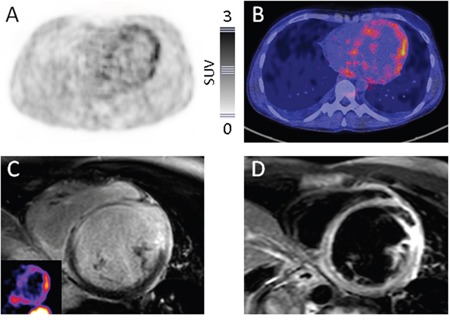
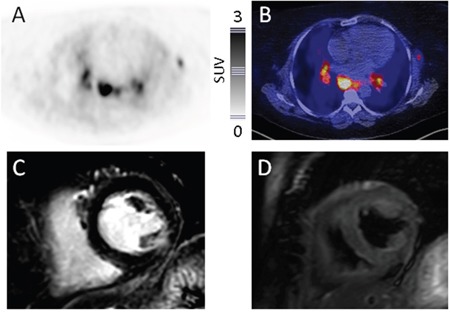
Diagnosis of cardiac sarcoidosis is often challenging. Whereas cardiac magnetic resonance imaging (CMR) and positron emission tomography/computed tomography (PET/CT) with 18F-fluorodeoxyglucose (FDG) are most commonly used to evaluate patients, PET/CT using radiolabeled somatostatin receptor (SSTR) ligands for visualization of inflammation might represent a more specific alternative. This study aimed to investigate the feasibility of SSTR-PET/CT for detecting cardiac sarcoidosis in comparison to CMR.15 patients (6 males, 9 females) with sarcoidosis and suspicion on cardiac involvement underwent SSTR-PET/CT imaging and CMR. Images were visually scored. The AHA 17-segment model of the left myocardium was used for localization and comparison of inflamed myocardium for both imaging modalities. In semi-quantitative analysis, mean (SUVmean) and maximum standardized uptake values (SUVmax) of affected myocardium were calculated and compared with both remote myocardium and left ventricular (LV) cavity.SSTR-PET was positive in 7/15, CMR in 10/15 patients. Of the 3 CMR+/PET- subjects, one patient with minor involvement (<25% of wall thickness in CMR) was missed by PET. The remaining two CMR+/PET- patients displayed no adverse cardiac events during follow-up.In the 17-segment model, PET/CT yielded 27 and CMR 29 positive segments. Overall concordance of the 2 modalities was 96.1% (245/255 segments analyzed). SUVmean and SUVmax in inflamed areas were 2.0±1.2 and 2.6±1.2, respectively. The lesion-to-remote myocardium and lesion-to-LV cavity ratios were 1.8±0.2 and 1.9±0.2 for SUVmean and 2.0±0.3 and 1.7±0.3 for SUVmax, respectively.Detection of cardiac sarcoidosis by SSTR-PET/CT is feasible. Our data warrant further analysis in larger prospective series.
Keywords: DOTATOC; PET; SSTR; sarcoidosis; somatostatin receptor.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
References
-
- Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H, Jr, Bresnitz EA, DePalo L, Hunninghake G, Iannuzzi MC, Johns CJ, McLennan G, Moller DR, Newman LS, et al. Clinical characteristics of patients in a case control study of sarcoidosis. American journal of respiratory and critical care medicine. 2001;164:1885–1889. - PubMed
-
- Mehta D, Lubitz SA, Frankel Z, Wisnivesky JP, Einstein AJ, Goldman M, Machac J, Teirstein A. Cardiac involvement in patients with sarcoidosis: diagnostic and prognostic value of outpatient testing. Chest. 2008;133:1426–1435. - PubMed
-
- Gideon NM, Mannino DM. Sarcoidosis mortality in the United States 1979-1991: an analysis of multiple-cause mortality data. The American journal of medicine. 1996;100:423–427. - PubMed
-
- Cooper LT, Baughman KL, Feldman AM, Frustaci A, Jessup M, Kuhl U, Levine GN, Narula J, Starling RC, Towbin J, Virmani R. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology Endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. European heart journal. 2007;28:3076–3093. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
