

Implementation of a pragmatic, stepped-wedge cluster randomized trial to evaluate impact of Botswana's Xpert MTB/RIF diagnostic algorithm on TB diagnostic sensitivity and early antiretroviral therapy mortality
- PMID: 27782821
- PMCID: PMC5080709
- DOI: 10.1186/s12879-016-1905-4
Implementation of a pragmatic, stepped-wedge cluster randomized trial to evaluate impact of Botswana's Xpert MTB/RIF diagnostic algorithm on TB diagnostic sensitivity and early antiretroviral therapy mortality
Abstract
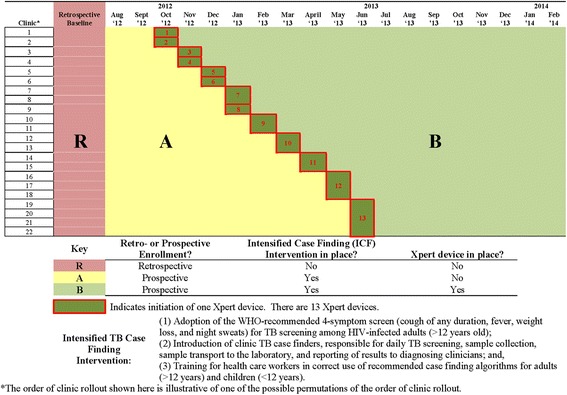
Background: In 2012, as a pilot for Botswana's national Xpert MTB/RIF (Xpert) rollout plans, intensified tuberculosis (TB) case finding (ICF) activities were strengthened at 22 HIV treatment clinics prior to phased activation of 13 Xpert instruments. Together, the strengthened ICF intervention and Xpert activation are referred to as the "Xpert package".
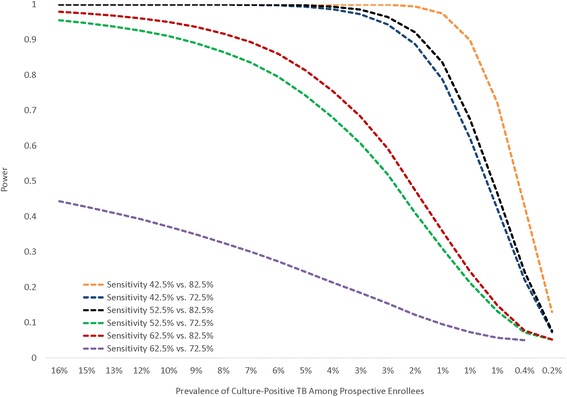
Methods: The evaluation, called the Xpert Package Rollout Evaluation using a Stepped-wedge design (XPRES), has two key objectives: (1) to compare sensitivity of microscopy-based and Xpert-based pulmonary TB diagnostic algorithms in diagnosing sputum culture-positive TB; and (2) to evaluate impact of the "Xpert package" on all-cause, 6-month, adult antiretroviral therapy (ART) mortality. A pragmatic, stepped-wedge cluster-randomized trial design was chosen. The design involves enrollment of three cohorts: (1) cohort R, a retrospective cohort of all study clinic ART enrollees in the 24 months before study initiation (July 31, 2012); (2) cohort A, a prospective cohort of all consenting patients presenting to study clinics after study initiation, who received the ICF intervention and the microscopy-based TB diagnostic algorithm; and (3) cohort B, a prospective cohort of all consenting patients presenting to study clinics after Xpert activation, who received the ICF intervention and the Xpert-based TB diagnostic algorithm. TB diagnostic sensitivity will be compared between TB culture-positive enrollees in cohorts A and B. All-cause, 6-month ART-mortality will be compared between cohorts R and B. With anticipated cohort R, A, and B sample sizes of about 10,131, 1,878, and 4,258, respectively, the study is estimated to have >80 % power to detect differences in pre-versus post-Xpert TB diagnostic sensitivity if pre-Xpert sensitivity is ≤52.5 % and post-Xpert sensitivity ≥82.5 %, and >80 % power to detect a 40 % reduction in all-cause, 6-month, ART mortality between cohorts R and B if cohort R mortality is ≥13/100 person-years.
Discussion: Only one small previous trial (N = 424) among ART enrolees in Zimbabwe evaluated, in a secondary analysis, Xpert impact on all-cause 6-month ART mortality. No mortality impact was observed. This Botswana trial, with its larger sample size and powered specifically to detect differences in all-cause 6-month ART mortality, remains well-positioned to contribute understanding of Xpert impact.
Trial registration: Retrospectively registered at ClinicalTrials.gov: NCT02538952 .
Keywords: Antiretroviral therapy; Botswana; Diagnostic accuracy; Mortality; People living with HIV; Sensitivity; Stepped-wedge cluster randomized trial; Xpert MTB/RIF.
Figures


References
-
- Cox JA, Lukande RL, Lucas S, Nelson AM, Van Marck E, Colebunders R. Autopsy causes of death in HIV-positive individuals in sub-Saharan Africa and correlation with clinical diagnoses. AIDS Rev. 2010;12(4):183–94. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
