

Increased mortality in hematological malignancy patients with acute respiratory failure from undetermined etiology: a Groupe de Recherche en Réanimation Respiratoire en Onco-Hématologique (Grrr-OH) study
- PMID: 27783381
- PMCID: PMC5080277
- DOI: 10.1186/s13613-016-0202-0
Increased mortality in hematological malignancy patients with acute respiratory failure from undetermined etiology: a Groupe de Recherche en Réanimation Respiratoire en Onco-Hématologique (Grrr-OH) study
Abstract
Background: Acute respiratory failure (ARF) is the most frequent complication in patients with hematological malignancies and is associated with high morbidity and mortality. ARF etiologies are numerous, and despite extensive diagnostic workflow, some patients remain with undetermined ARF etiology.
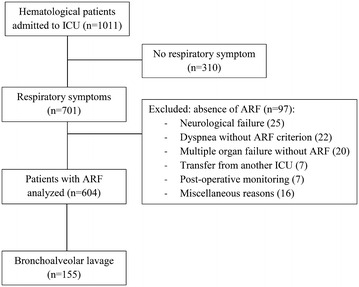
Methods: This is a post-hoc study of a prospective multicenter cohort performed on 1011 critically ill hematological patients. Relationship between ARF etiology and hospital mortality was assessed using a multivariable regression model adjusting for confounders.
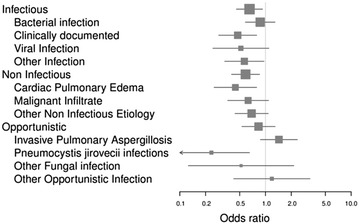
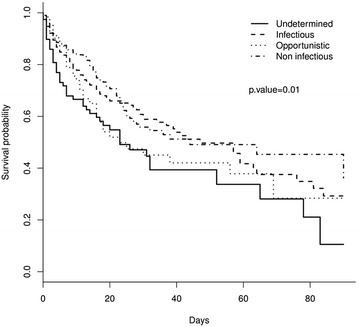
Results: This study included 604 patients with ARF. All patients underwent noninvasive diagnostic tests, and a bronchoscopy and bronchoalveolar lavage (BAL) was performed in 155 (25.6%). Definite diagnoses were classified into four exclusive etiological categories: pneumonia (44.4%), non-infectious diagnoses (32.6%), opportunistic infection (10.1%) and undetermined (12.9%), with corresponding hospital mortality rates of 40, 35, 55 and 59%, respectively. Overall hospital mortality was 42%. By multivariable analysis, factors associated with hospital mortality were invasive pulmonary aspergillosis (OR 7.57 (95% CI 3.06-21.62); p < 0.005), use of invasive mechanical ventilation (OR 1.65 (95% CI 1.07-2.55); p = 0.02), a SOFA score >7 (OR 3.32 (95% CI 2.15-5.15); p < 0.005) and an undetermined ARF etiology (OR 2.92 (95% CI 1.71-5.07); p < 0.005).
Conclusions: In patients with hematological malignancies and ARF, up to 13% remain with undetermined ARF etiology despite comprehensive diagnostic workup. Undetermined ARF etiology is independently associated with hospital mortality. Studies to guide second-line diagnostic strategies are warranted. ClinicalTrials.Gov NCT01172132.
Keywords: Acute respiratory failure; Bronchoalveolar lavage; Diagnostic strategy; Etiologies; Hematological malignancies; Outcome.
Figures

References
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
