

The Relationship between Active Trachoma and Ocular Chlamydia trachomatis Infection before and after Mass Antibiotic Treatment
- PMID: 27783678
- PMCID: PMC5082620
- DOI: 10.1371/journal.pntd.0005080
The Relationship between Active Trachoma and Ocular Chlamydia trachomatis Infection before and after Mass Antibiotic Treatment
Abstract
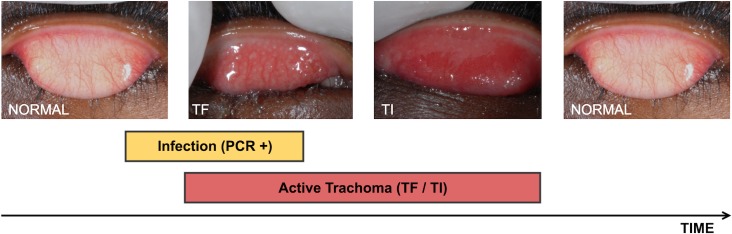
Background: Trachoma is a blinding disease, initiated in early childhood by repeated conjunctival infection with the obligate intracellular bacterium Chlamydia trachomatis. The population prevalence of the clinical signs of active trachoma; ''follicular conjunctivitis" (TF) and/or ''intense papillary inflammation" (TI), guide programmatic decisions regarding the initiation and cessation of mass drug administration (MDA). However, the persistence of TF following resolution of infection at both the individual and population level raises concerns over the suitability of this clinical sign as a marker for C. trachomatis infection.
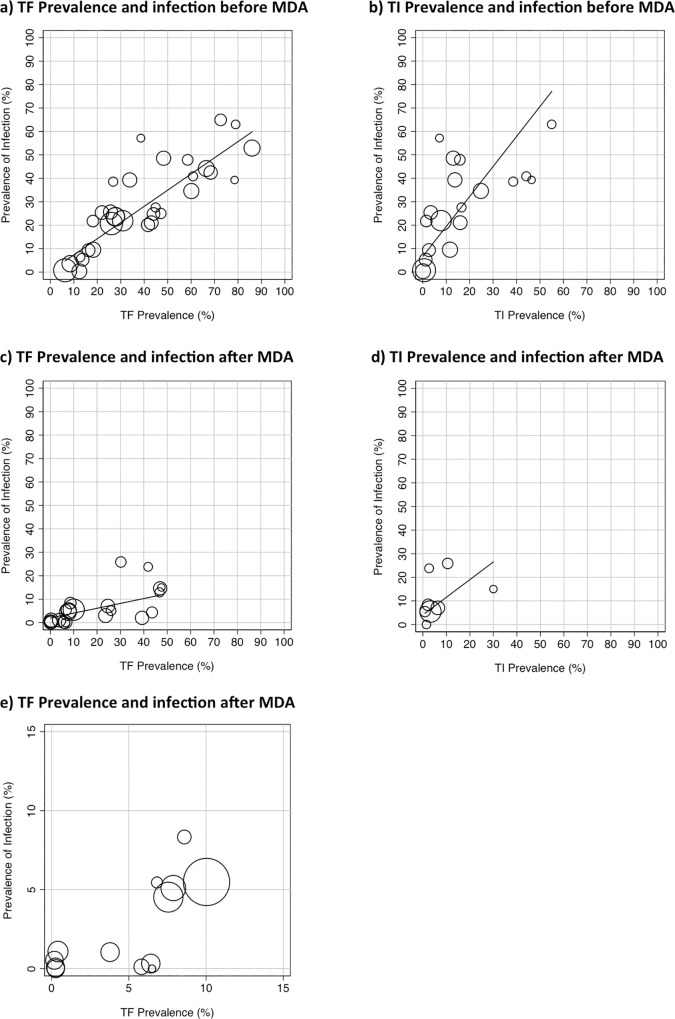
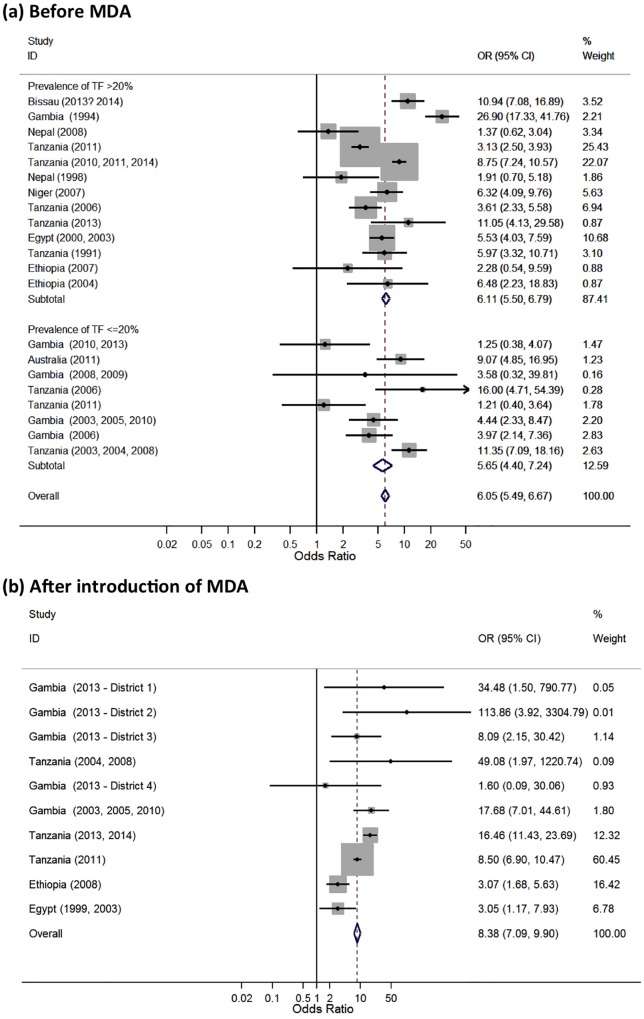
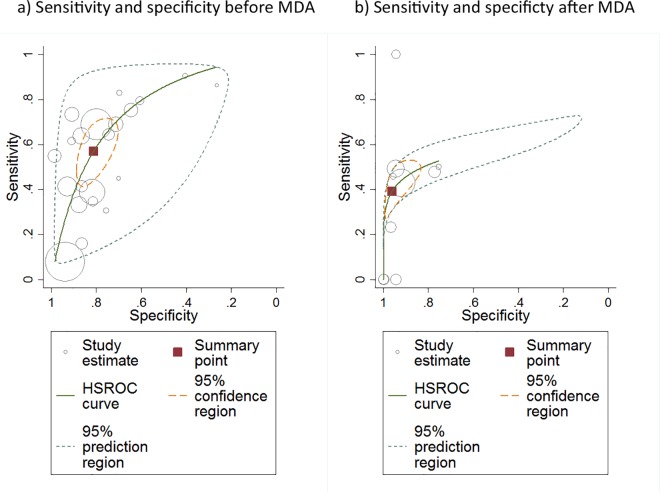
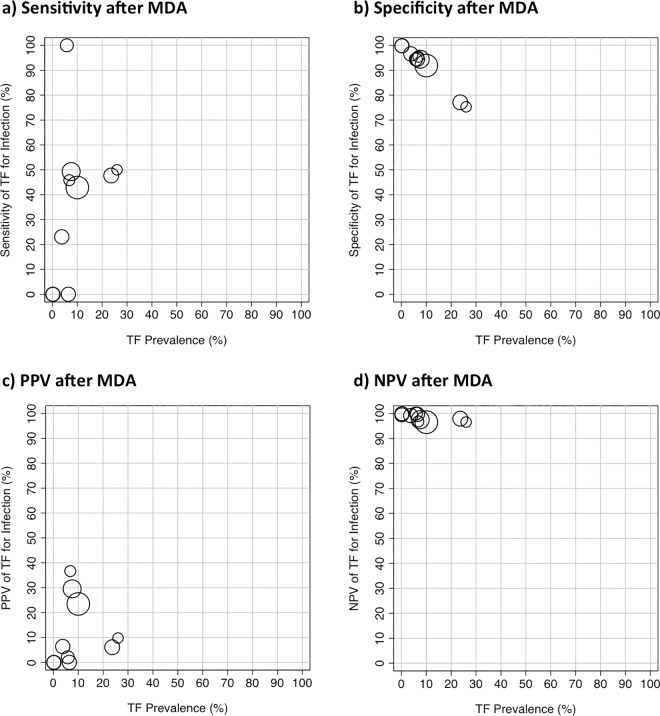
Methodology/principle findings: We systematically reviewed the literature for population-based studies and those including randomly selected individuals, which reported the prevalence of the clinical signs of active trachoma and ocular C. trachomatis infection by nucleic acid amplification test. We performed a meta-analysis to assess the relationship between active trachoma and C. trachomatis infection before and after MDA. TF and C. trachomatis infection were strongly correlated prior to MDA (r = 0.92, 95%CI 0.83 to 0.96, p<0.0001); the relationship was similar when the analysis was limited to children. A moderate correlation was found between TI and prevalence of infection. Following MDA, the relationship between TF and infection prevalence was weaker (r = 0.60, 95%CI 0.25 to 0.81, p = 0.003) and there was no correlation between TI and C. trachomatis infection.
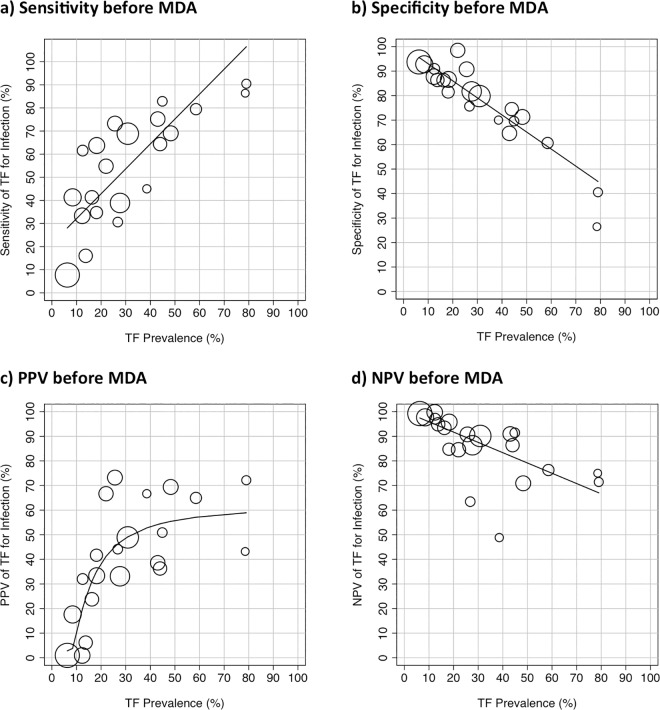
Conclusions/significance: Prior to MDA, TF is a good indicator of the community prevalence of C. trachomatis infection. Following MDA, the prevalence of TF tends to overestimate the underlying infection prevalence. In order to prevent unnecessary additional rounds of MDA and to accurately ascertain when elimination goals have been reached, a cost-effective test for C. trachomatis that can be administered in low-resource settings remains desirable.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Taylor HR, Burton MJ, Haddad D, West S, Wright H. Trachoma. Lancet (London, England). 2014;384(9960):2142–52. Epub 2014/07/22. - PubMed
-
- Jawetz E, Rose L, Hanna L, Thygeson P. Experimental inclusion conjunctivitis in man: measurements of infectivity and resistance. Jama. 1965;194(6):620–32. Epub 1965/11/08. - PubMed
-
- Bailey RL, Holland MJ, Whittle HC, Mabey DC. Subjects recovering from human ocular chlamydial infection have enhanced lymphoproliferative responses to chlamydial antigens compared with those of persistently diseased controls. Infection and immunity. 1995;63(2):389–92. Epub 1995/02/01. PubMed Central PMCID: PMCPMC173007. - PMC - PubMed
-
- Grassly NC, Ward ME, Ferris S, Mabey DC, Bailey RL. The natural history of trachoma infection and disease in a Gambian cohort with frequent follow-up. PLoS neglected tropical diseases. 2008;2(12):e341 Epub 2008/12/03. PubMed Central PMCID: PMCPMC2584235. 10.1371/journal.pntd.0000341 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
