

Association Between Medicare Hospital Readmission Penalties and 30-Day Combined Excess Readmission and Mortality
- PMID: 27784054
- PMCID: PMC5503688
- DOI: 10.1001/jamacardio.2016.3704
Association Between Medicare Hospital Readmission Penalties and 30-Day Combined Excess Readmission and Mortality
Abstract
Importance: US hospitals receive financial penalties for excess risk-standardized 30-day readmissions and mortality in Medicare patients. Under current policy, readmission prevention is incentivized over 10-fold more than mortality reduction.
Objective: To determine how penalties for US hospitals would change if policy equally weighted 30-day readmissions and mortality.
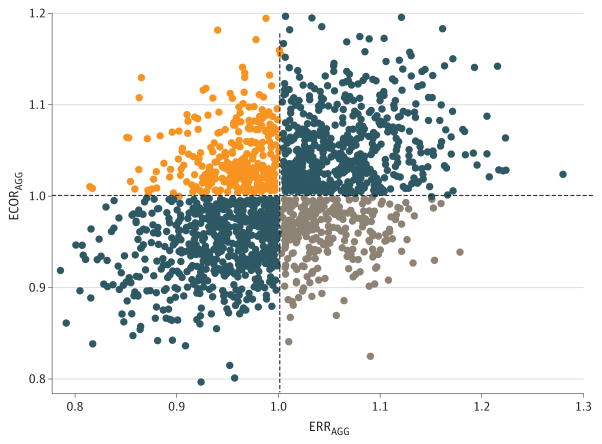
Design, setting, and participants: Publicly available hospital-level data for fiscal year 2014 was obtained, including excess readmission ratio (ERR; risk-standardized predicted over expected 30-day readmissions) and 30-day mortality rates for heart failure, pneumonia, and acute myocardial infarction, as well as readmission penalties (as percent of Medicare Diagnosis Group payments). An excess mortality ratio (EMR) was calculated by dividing the risk-standardized predicted mortality by the national average mortality. Case-weighted aggregate ERR (ERRAGG) and EMR (EMRAGG) were calculated, and an excess combined outcome ratio (ECORAGG) was created by averaging ERRAGG and EMRAGG. We examined associations between readmission penalties, ERRAGG, EMRAGG, and ECORAGG. Analysis of variance was used to compare readmission penalties in hospitals with concordant (both ratios >1 or <1) and discordant performance by ERRAGG and ECORAGG.
Main outcomes and measures: The primary outcome investigated was the association between readmission penalties and the calculated excess combined outcome ratio (ECORAGG).
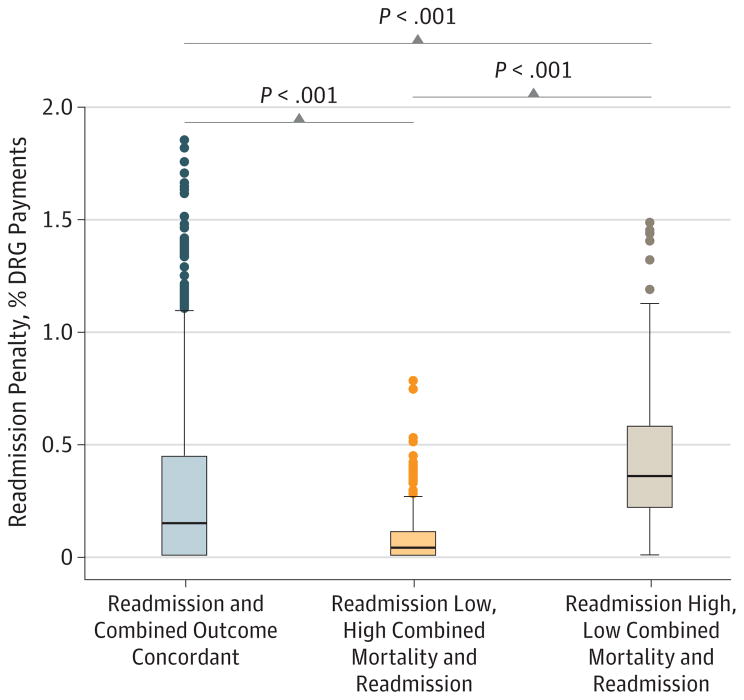
Results: In 1963 US hospitals with complete data, readmission penalties closely tracked excess readmissions (r = 0.81; P < .001), but were minimally and inversely related with excess mortality (r = -0.12; P < .001) and only modestly correlated with excess combined readmission and mortality (r = 0.36; P < .001). Using hospitals with concordant ERRAGG and ECORAGG as the reference group, 17% of hospitals had an ECORAGG ratio less than 1 (ie, superior combined mortality/readmission outcome) with an ERRAGG ratio greater than 1, and received higher mean (SD) readmission penalties (0.41% [0.28%] vs 0.29% [0.37%]; P < .001); 16% of US hospitals had an ECORAGG ratio of greater than 1 (ie, inferior combined mortality/readmission outcome) with an ERRAGG ratio less than 1, and received minimal mean (SD) readmission penalties (0.08% [0.12%]; P < .001 for comparison with reference).
Conclusions and relevance: In fiscal year 2014, financial penalties for one-third of US hospitals would have been substantially altered if 30-day readmission and mortality were considered equally important. Under most circumstances, patients would rather avoid death than rehospitalization. Current Medicare financial penalties do not meet the goals of aligning incentives and fairly reimbursing hospitals for patient-centered outcomes.
Figures
References
-
- Medicare.gov. [Accessed April 17, 2016];Hospital Compare Datasets. https://data.medicare.gov//data/hospital-compare.
-
- Medicare Readmission Penalties by Hospital. [Accessed April 17, 2016];Kaiser Health News. https://kaiserhealthnews.files.wordpress.com/2013/08/readmission-year-2-....
-
- Medicare.gov. Hospital Compare. [Accessed July 8, 2016];Linking quality to payment. https://www.medicare.gov/hospitalcompare/linking-quality-to-payment.html.
-
- Centers for Medicare and Medicaid Services. [Accessed July 15, 2016];Hospital Quality Initiative Measure Methodology. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Inst....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
