

Longitudinal Study of Postconcussion Syndrome: Not Everyone Recovers
- PMID: 27784191
- PMCID: PMC5397249
- DOI: 10.1089/neu.2016.4677
Longitudinal Study of Postconcussion Syndrome: Not Everyone Recovers
Abstract
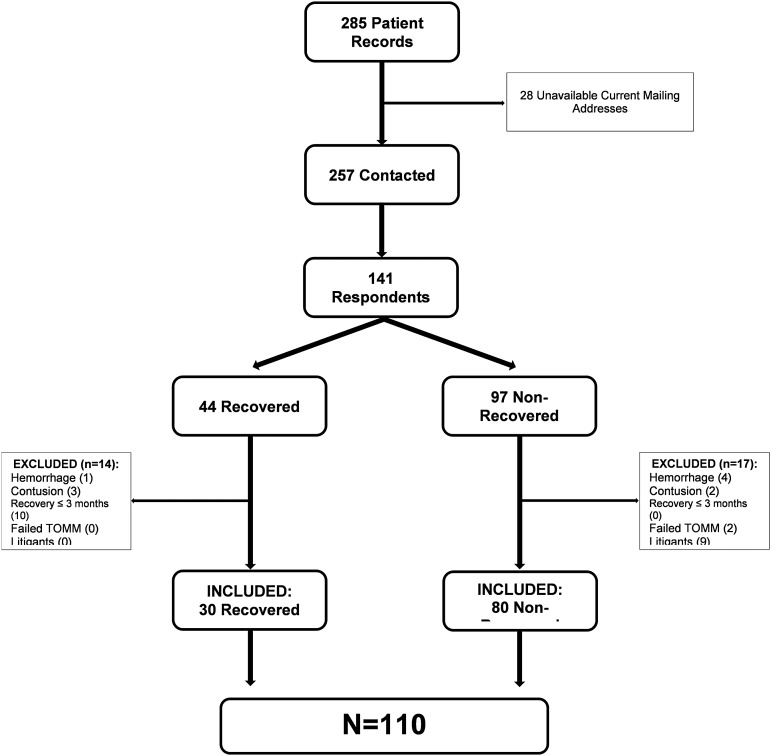
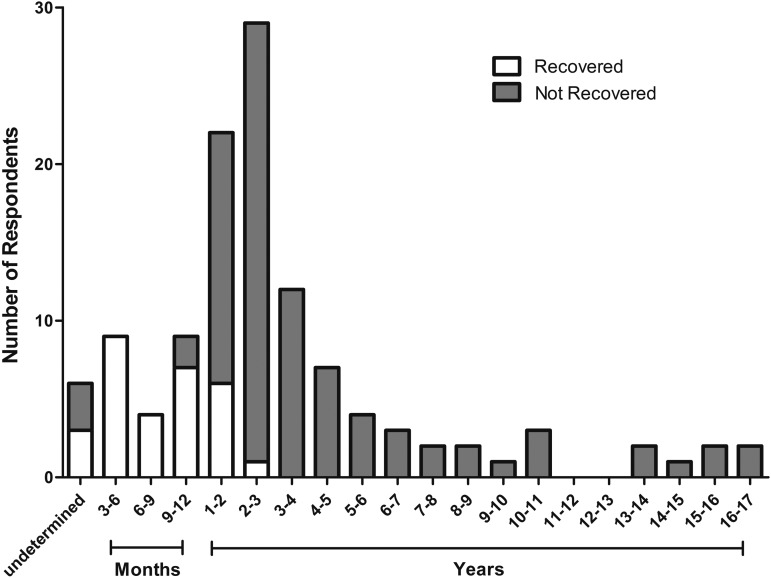
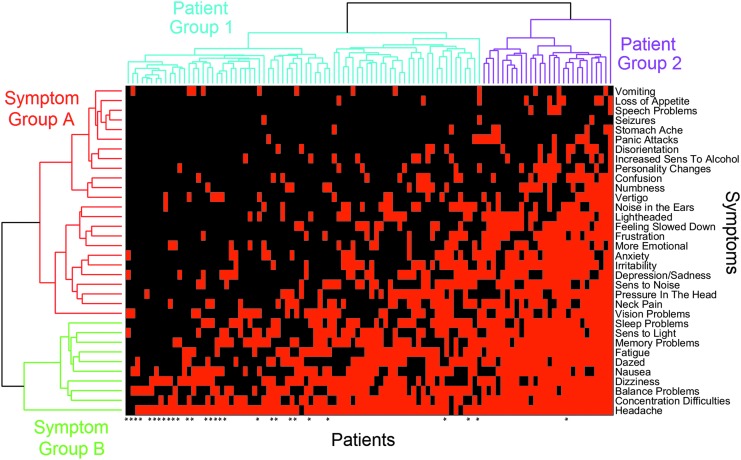
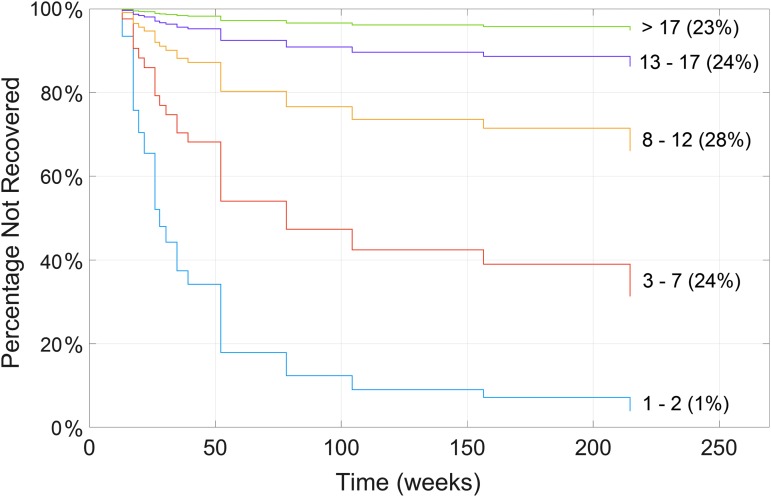
We examined recovery from postconcussion syndrome (PCS) in a series of 285 patients diagnosed with concussion based on international sport concussion criteria who received a questionnaire regarding recovery. Of 141 respondents, those with postconcussion symptoms lasting less than 3 months, a positive computed tomography (CT) and/or magnetic resonance imaging (MRI), litigants, and known Test of Memory Malingering (TOMM)-positive cases were excluded, leaving 110 eligible respondents. We found that only 27% of our population eventually recovered and 67% of those who recovered did so within the first year. Notably, no eligible respondent recovered from PCS lasting 3 years or longer. Those who did not recover (n = 80) were more likely to be non-compliant with a do-not-return-to-play recommendation (p = 0.006) but did not differ from the recovered group (n = 30) in other demographic variables, including age and sex (p ≥ 0.05). Clustergram analysis revealed that symptoms tended to appear in a predictable order, such that symptoms later in the order were more likely to be present if those earlier in the order were already present. Cox proportional hazards model analysis showed that the more symptoms reported, the longer the time to recovery (p = 7.4 × 10-6), with each additional symptom reducing the recovery rate by approximately 20%. This is the first longitudinal PCS study to focus on PCS defined specifically as a minimum of 3 months of symptoms, negative CT and/or MRI, negative TOMM test, and no litigation. PCS may be permanent if recovery has not occurred by 3 years. Symptoms appear in a predictable order, and each additional PCS symptom reduces recovery rate by 20%. More long-term follow-up studies are needed to examine recovery from PCS.
Keywords: definitions, eligibility, and exclusions; number of symptoms; postconcussion syndrome; recovery.
Conflict of interest statement
No competing financial interests exist.
Figures

References
-
- Bazarian J.J., Wong T., Harris M., Leahey N., Mookerjee S., and Dombovy M. (1999). Epidemiology and predictors of post-concussive syndrome after minor head injury in an emergency population. Brain Inj. 13, 173–189 - PubMed
-
- Iverson G.L. (2005). Outcome from mild traumatic brain injury. Curr. Opin. Psychiatry 18, 301–317 - PubMed
-
- Makdissi M., Cantu R.C., Johnston K.M., McCrory P., and Meeuwisse W.H. (2013). The difficult concussion patient: what is the best approach to investigation and management of persistent (>10 days) postconcussive symptoms? Br. J. Sports Med. 47, 308–313 - PubMed
-
- Carroll L.J., Cassidy J.D., Holm L., Kraus J., and Coronado V.G.; WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. (2004). Methodological issues and research recommendations for mild traumatic brain injury: the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J. Rehabil. Med. 113–125 - PubMed
-
- Zemek R.L., Farion K.J., Sampson M., and McGahern C. (2013). Prognosticators of persistent symptoms following pediatric concussion: a systematic review. JAMA Pediatr. 167, 259–265 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
