

Ready-Made Versus Custom-Made Mandibular Repositioning Devices in Sleep Apnea: A Randomized Clinical Trial
- PMID: 27784410
- PMCID: PMC5263072
- DOI: 10.5664/jcsm.6440
Ready-Made Versus Custom-Made Mandibular Repositioning Devices in Sleep Apnea: A Randomized Clinical Trial
Abstract
Study objectives: To compare the effectiveness of a custom-made (MRDc) versus ready-made (MRDr) mandibular repositioning devices (MRD) in the management of obstructive sleep apnea (OSA).
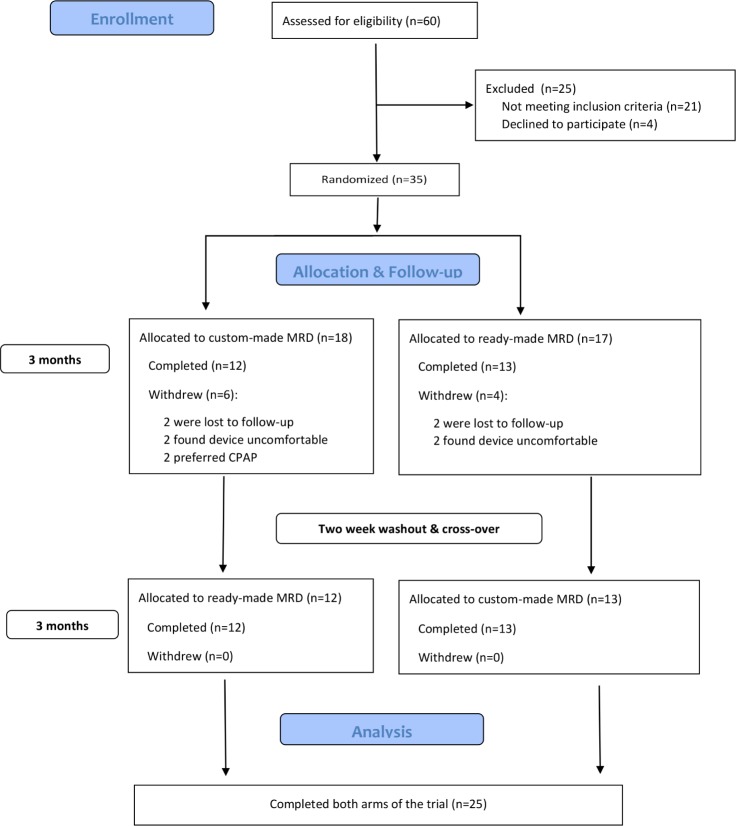
Methods: A randomized crossover trial design was adopted in which patients with a confirmed diagnosis of OSA were randomly allocated to receive either a 3-month period of ready-made or custom-made MRD, with an intervening washout period of 2 weeks, prior to crossover. Treatment outcomes included both objective sleep monitoring and patient-centered measures (daytime sleepiness, partner snoring and quality of life).
Results: Twenty-five patients, with a mild degree of OSA (apnea-hypopnea index of 13.3 [10.9-25] events/h) and daytime sleepiness (Epworth Sleepiness Scale of 11 [6-16]), completed both arms of the trial. The MRDc achieved a complete treatment response in 64% of participants, compared with 24% with the MRDr (p < 0.001). A significant difference was observed in treatment failures, when comparing the MRDr (36%) with the MRDc (4%). Excessive daytime sleepiness (Epworth Sleepiness Scale ≥ 10) persisted in 33% (MRDc) and 66% (MRDr) of OSA subjects, following treatment. A statistically significant improvement was observed in quality of life scales following MRDc therapy only. Significant differences were observed in relation to both the number of nights per week (p = 0.004) and hours per night (p = 0.006) between the two different designs of device.
Conclusions: The study demonstrates the significant clinical effectiveness of a custom-made mandibular repositioning device, particularly in terms of patient compliance and tolerance, in the treatment of OSA.
Keywords: appliance; clinical studies; clinical trial; sleep disorders; therapy.
© 2017 American Academy of Sleep Medicine
Figures

Similar articles
-
Oral Appliance Therapy in Patients With Daytime Sleepiness and Snoring or Mild to Moderate Sleep Apnea: A Randomized Clinical Trial.JAMA Intern Med. 2015 Aug;175(8):1278-85. doi: 10.1001/jamainternmed.2015.2051. JAMA Intern Med. 2015. PMID: 26030264 Clinical Trial.
-
Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial.Am J Respir Crit Care Med. 2013 Apr 15;187(8):879-87. doi: 10.1164/rccm.201212-2223OC. Am J Respir Crit Care Med. 2013. PMID: 23413266 Clinical Trial.
-
Snoring and Obstructive Sleep Apnea: Objective Efficacy and Impact of a Chairside Fabricated Mandibular Advancement Device.J Prosthodont. 2017 Jul;26(5):381-386. doi: 10.1111/jopr.12401. Epub 2015 Nov 30. J Prosthodont. 2017. PMID: 26619077 Clinical Trial.
-
Ready-made versus custom-made mandibular advancement appliances in obstructive sleep apnea: A systematic review and meta-analysis.J Sleep Res. 2018 Dec;27(6):e12660. doi: 10.1111/jsr.12660. Epub 2018 Feb 6. J Sleep Res. 2018. PMID: 29405512
-
Non-CPAP therapies in obstructive sleep apnoea: mandibular advancement device therapy.Eur Respir J. 2012 May;39(5):1241-7. doi: 10.1183/09031936.00144711. Epub 2011 Nov 10. Eur Respir J. 2012. PMID: 22075487 Review.
Cited by
-
Comparative assessment of changes in pharyngeal airway space in cases of obstructive sleep apnoea with a customized mandibular repositioning appliance - a clinical study.Sleep Sci. 2021 Jan-Mar;14(Spec 1):16-24. doi: 10.5935/1984-0063.20200072. Sleep Sci. 2021. PMID: 34917269 Free PMC article.
-
Three Decades of Managing Pediatric Obstructive Sleep Apnea Syndrome: What's Old, What's New.Children (Basel). 2025 Jul 11;12(7):919. doi: 10.3390/children12070919. Children (Basel). 2025. PMID: 40723112 Free PMC article. Review.
-
Factors influencing adherence to oral appliance therapy in adults with obstructive sleep apnea: a systematic review and meta-analysis.J Clin Sleep Med. 2021 Jul 1;17(7):1485-1498. doi: 10.5664/jcsm.9184. J Clin Sleep Med. 2021. PMID: 33660611 Free PMC article.
-
Mandibular Advancement Device Treatment Efficacy Is Associated with Polysomnographic Endotypes.Ann Am Thorac Soc. 2021 Mar;18(3):511-518. doi: 10.1513/AnnalsATS.202003-220OC. Ann Am Thorac Soc. 2021. PMID: 32946702 Free PMC article. Clinical Trial.
-
Mandibular Advancement Splint Therapy.Adv Exp Med Biol. 2022;1384:373-385. doi: 10.1007/978-3-031-06413-5_22. Adv Exp Med Biol. 2022. PMID: 36217096
References
-
- Pataka A, Riha RL. Continuous positive airway pressure and cardiovascular events in patients with obstructive sleep apnea. Curr Cardiol Rep. 2013;15(8):385. - PubMed
-
- Continuous positive airway pressure for the treatment of obstructive sleep apnoea/hypopnoea syndrome. National Institute for Health and Care Excellence Web site. [Accessed January 5, 2017]. https://www.nice.org.uk/guidance/ta139. Published March 26, 2008.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
