

Predicting survival after acute civilian penetrating brain injuries: The SPIN score
- PMID: 27784772
- PMCID: PMC5123553
- DOI: 10.1212/WNL.0000000000003355
Predicting survival after acute civilian penetrating brain injuries: The SPIN score
Abstract
Objective: To identify predictors associated with survival in civilian penetrating traumatic brain injury (pTBI) utilizing a contemporary, large, diverse 2-center cohort, and to develop a parsimonious survival prediction score for pTBI.
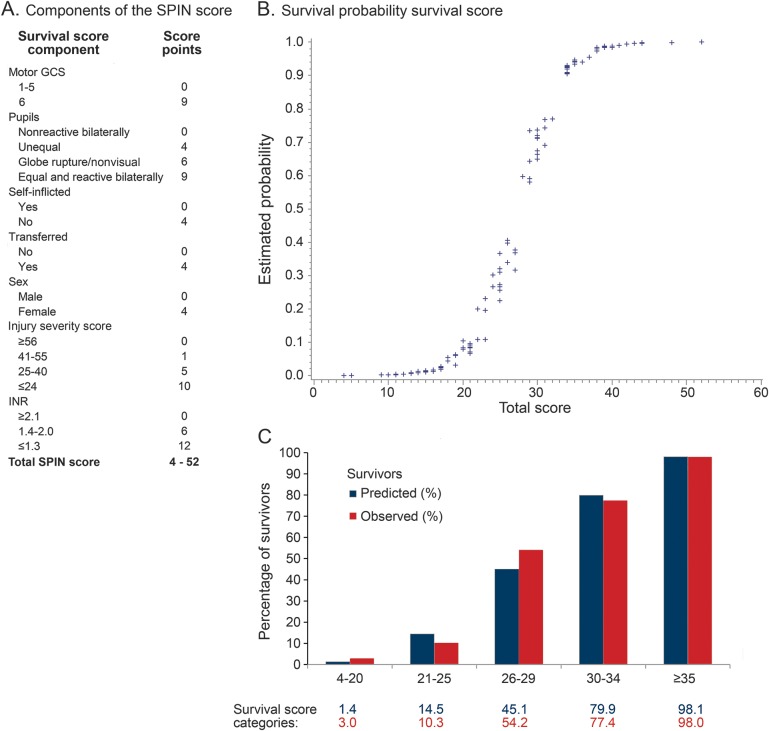
Methods: Our cohort comprised 413 pTBI patients retrospectively identified from the local trauma registries at 2 US level 1 trauma centers, of which one was predominantly urban and the other predominantly rural. Predictors of in-hospital and 6-month survival identified in univariate and multivariable logistic regression were used to develop the simple Surviving Penetrating Injury to the Brain (SPIN) score.
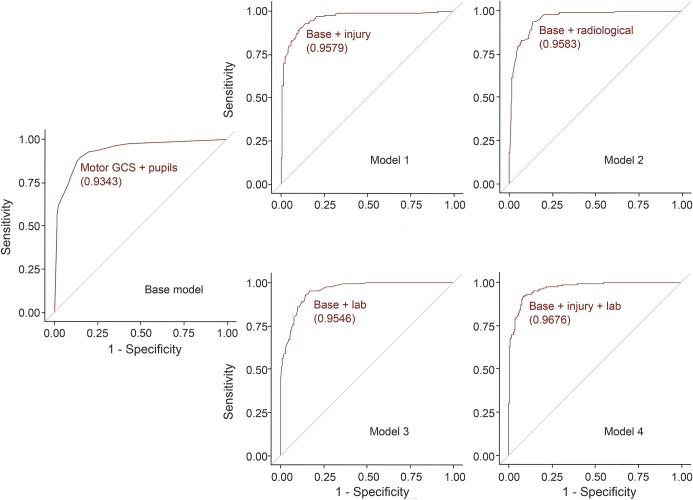
Results: The mean age was 33 ± 16 years and patients were predominantly male (87%). Survival at hospital discharge as well as 6 months post pTBI was 42.4%. Higher motor Glasgow Coma Scale subscore, pupillary reactivity, lack of self-inflicted injury, transfer from other hospital, female sex, lower Injury Severity Score, and lower international normalized ratio were independently associated with survival (all p < 0.001; model area under the curve 0.962). Important radiologic factors associated with survival were also identified but their addition to the full multivariable would have resulted in model overfitting without much gain in the area under the curve.
Conclusions: The SPIN score, a logistic regression-based clinical risk stratification scale estimating survival after pTBI, was developed in this large, diverse 2-center cohort. While this preliminary clinical survival prediction tool does not include radiologic factors, it may support clinical decision-making after civilian pTBI if external validation confirms the probability estimates.
© 2016 American Academy of Neurology.
Figures
References
-
- Aldrich EF, Eisenberg HM, Saydjari C, et al. Predictors of mortality in severely head-injured patients with civilian gunshot wounds: a report from the NIH Traumatic Coma Data Bank. Surg Neurol 1992;38:418–423. - PubMed
-
- Aarabi B, Tofighi B, Kufera JA, et al. Predictors of outcome in civilian gunshot wounds to the head. J Neurosurg 2014;120:1138–1146. - PubMed
-
- Martins RS, Siqueira MG, Santos MT, Zanon-Collange N, Moraes OJ. Prognostic factors and treatment of penetrating gunshot wounds to the head. Surg Neurol 2003;60:98–104; discussion 104. - PubMed
-
- Joseph B, Aziz H, Pandit V, et al. Improving survival rates after civilian gunshot wounds to the brain. J Am Coll Surg 2014;218:58–65. - PubMed
-
- Gressot LV, Chamoun RB, Patel AJ, et al. Predictors of outcome in civilians with gunshot wounds to the head upon presentation. J Neurosurg 2014;121:645–652. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources