

Combined Placement of Covered Self-Expanding Metallic Stents and Nasojejunal Tube for Managing Large Lower Esophageal Perforations
- PMID: 27785265
- PMCID: PMC5051138
- DOI: 10.14740/gr593w
Combined Placement of Covered Self-Expanding Metallic Stents and Nasojejunal Tube for Managing Large Lower Esophageal Perforations
Abstract
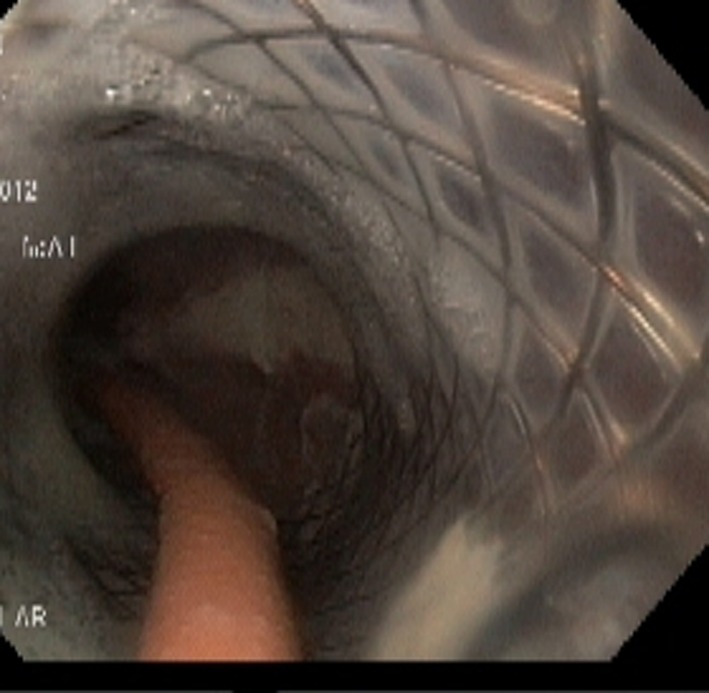
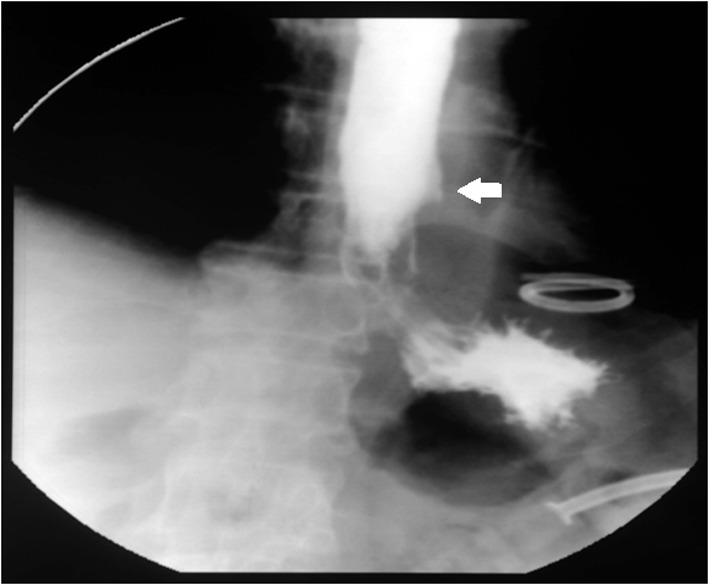
Covered self-expanding metallic stents (cSEMSs) have emerged as effective treatment option for esophageal perforations. However, the large lower esophageal perforations where the cSEMS is placed across gastroesophageal junction have lower healing rates because refluxed gastric contents constantly irritate perforation and also there is increased risk of stent migration. Moreover, gastric mucosa tends to prolapse into lumen of lower end of stent causing its obstruction, leading to seepage of saliva and fluids from upper end of stent even in the patients who are on parenteral nutrition. We present our experience of a novel technique of combined cSEMS and nasojejunal tube (NJT) placement in four patients (two males) with benign large lower esophageal perforations. The NJT was placed through the stent into the jejunum through which patients were given enteral feeding. The stents were placed 5 - 21 days after esophageal perforation with the size of perforation ranging from 4 to 6 cm. As the NJT formed a loop in stomach, it prevented migration of stent. And also its presence in lumen of stent prevented its obstruction by prolapsing gastric mucosa, thereby preventing seepage of saliva and fluids from side of stent. Both stents and NJT were removed after 6 weeks and leak closed in all patients. Combined cSEMS and NJT placement seems to be safe and effective for treating large lower esophageal perforations. NJT placement seems to decrease risk of migration, prevents seepage of fluids and permits early enteral nutrition, thereby improving the healing rates.
Keywords: Bariatric surgery; Esophagus; Leaks; Stents.
Figures






Similar articles
-
The role of esophageal stents in the management of esophageal anastomotic leaks and benign esophageal perforations.Ann Surg. 2014 May;259(5):852-60. doi: 10.1097/SLA.0000000000000564. Ann Surg. 2014. PMID: 24509201 Review.
-
Clinical outcomes following self-expanding metal stent placement for esophageal salvage.J Thorac Cardiovasc Surg. 2017 Sep;154(3):1145-1150. doi: 10.1016/j.jtcvs.2017.03.051. Epub 2017 Mar 23. J Thorac Cardiovasc Surg. 2017. PMID: 28416335
-
Endoscopic treatment of thoracic esophageal anastomotic leaks by using silicone-covered, self-expanding polyester stents.Gastrointest Endosc. 2005 Jun;61(7):891-6. doi: 10.1016/s0016-5107(05)00325-1. Gastrointest Endosc. 2005. PMID: 15933696
-
Utility of removable esophageal covered self-expanding metal stents for leak and fistula management.Ann Thorac Surg. 2010 Mar;89(3):931-6; discussion 936-7. doi: 10.1016/j.athoracsur.2009.10.061. Ann Thorac Surg. 2010. PMID: 20172156
-
Regulating migration of esophageal stents - management using a Sengstaken-Blakemore tube: A case report and review of literature.World J Gastroenterol. 2018 Jul 28;24(28):3192-3197. doi: 10.3748/wjg.v24.i28.3192. World J Gastroenterol. 2018. PMID: 30065565 Free PMC article. Review.
Cited by
-
Management of an Esophago-pleural Fistula after Emergent Endoscopic Variceal Injectional Sclerotherapy: A Case Report And Literature Review.Intern Med. 2024 Apr 1;63(7):937-941. doi: 10.2169/internalmedicine.1961-23. Epub 2023 Aug 16. Intern Med. 2024. PMID: 37587038 Free PMC article. Review.
References
-
- Bufkin BL, Miller JI Jr, Mansour KA. Esophageal perforation: emphasis on management. Ann Thorac Surg. 1996;61(5):1447–1451. discussion 1451-1442. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials