

The single surgeon learning curve of laparoscopic liver resection: A continuous evolving process through stepwise difficulties
- PMID: 27787369
- PMCID: PMC5089098
- DOI: 10.1097/MD.0000000000005138
The single surgeon learning curve of laparoscopic liver resection: A continuous evolving process through stepwise difficulties
Abstract
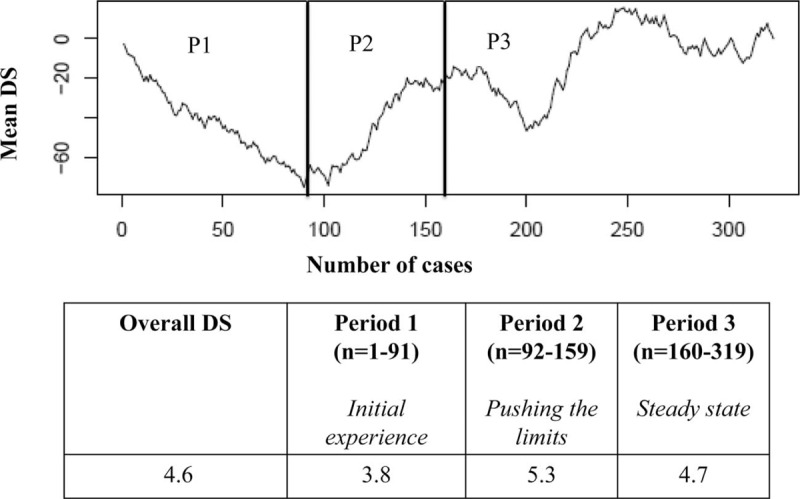
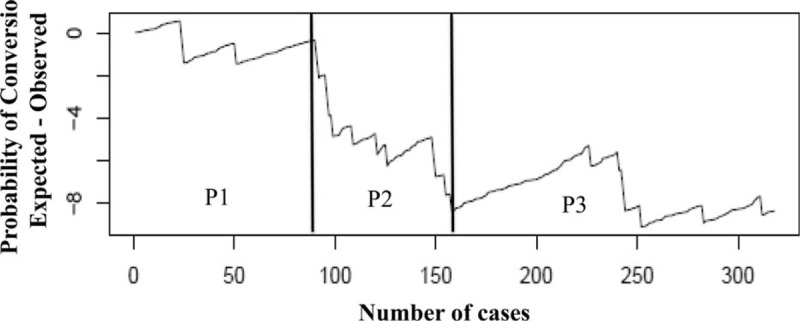
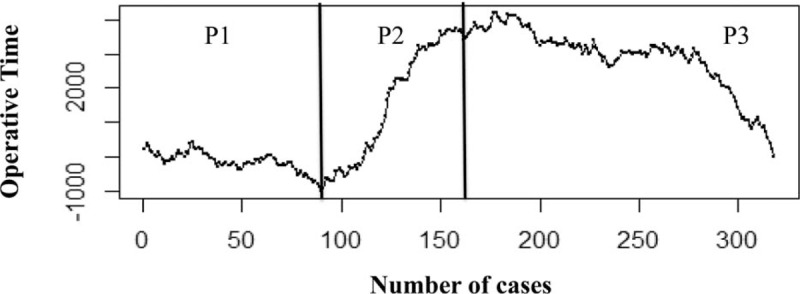
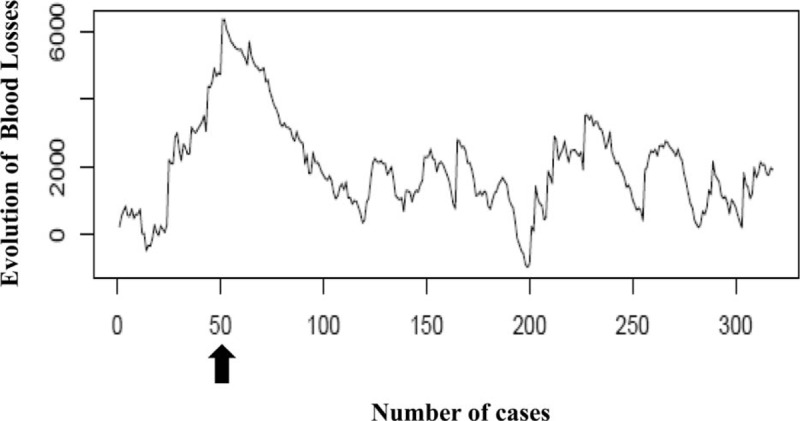
The aim of the study was to evaluate the single-surgeon learning curve (SSLC) in laparoscopic liver surgery over an 11-year period with risk-adjusted (RA) cumulative sum control chart analysis.Laparoscopic liver resection (LLR) is a challenging and highly demanding procedure. No specific data are available for defining the feasibility and reproducibility of the SSLC regarding a consistent and consecutive caseload volume over a specified time period.A total of 319 LLR performed by a single surgeon between June 2003 and May 2014 were retrospectively analyzed. A difficulty scale (DS) ranging from 1 to 10 was created to rate the technical difficulty of each LLR. The risk-adjusted cumulative sum control chart (RA-CUSUM) analysis evaluated conversion rate (CR), operative time (OT) and blood loss (BL). Perioperative morbidity and mortality were also analyzed.The RA-CUSUM analysis of the DS identified 3 different periods: P1 (n = 91 cases), with a mean DS of 3.8; P2 (cases 92-159), with a mean DS of 5.3; and P3 (cases 160-319), with a mean DS of 4.7. P2 presented the highest conversion and morbidity rates with a longer OT, whereas P3 showed the best results (P < 0.001). Fifty cases were needed to achieve a significant decrease in BL. The overall morbidity rate was 13.8%; no perioperative mortality was observed.According to our analysis, at least 160 cases (P3) are needed to complete the SSLC performing safely different types of LLR. A minimum of 50 cases can provide a significant decrease in BL. Based on these findings, a longer learning curve should be anticipated to broaden the indications for LLR.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Evaluating the learning curve for laparoscopic liver resection: a comparative study between standard and learning curve CUSUM.HPB (Oxford). 2019 Nov;21(11):1505-1512. doi: 10.1016/j.hpb.2019.03.362. Epub 2019 Apr 13. HPB (Oxford). 2019. PMID: 30992198
-
The learning curve of laparoscopic liver resection after the Louisville statement 2008: Will it be more effective and smooth?Surg Endosc. 2016 Jul;30(7):2895-903. doi: 10.1007/s00464-015-4575-1. Epub 2015 Oct 20. Surg Endosc. 2016. PMID: 26487203
-
Learning curve of self-taught laparoscopic liver surgeons in left lateral sectionectomy: results from an international multi-institutional analysis on 245 cases.Surg Endosc. 2016 Aug;30(8):3618-29. doi: 10.1007/s00464-015-4665-0. Epub 2015 Nov 16. Surg Endosc. 2016. PMID: 26572765
-
The learning curve in laparoscopic major liver resection.J Hepatobiliary Pancreat Sci. 2013 Feb;20(2):131-6. doi: 10.1007/s00534-012-0571-1. J Hepatobiliary Pancreat Sci. 2013. PMID: 23064988 Review.
-
Critical appraisal of the learning curve of minimally invasive hepatectomy: experience with the first 200 cases of a Southeast Asian early adopter.ANZ J Surg. 2020 Jun;90(6):1092-1098. doi: 10.1111/ans.15683. Epub 2020 Jan 20. ANZ J Surg. 2020. PMID: 31957149 Review.
Cited by
-
Advantages of laparoscopic left hemihepatectomy: A meta-analysis.Medicine (Baltimore). 2019 Jun;98(23):e15929. doi: 10.1097/MD.0000000000015929. Medicine (Baltimore). 2019. PMID: 31169712 Free PMC article.
-
A systematic surgical procedure: The '7+3' approach to laparoscopic right partial hepatectomy [deep segment (S) VI, S VII or S VIII] in 52 patients with liver tumors.Oncol Lett. 2018 May;15(5):7846-7854. doi: 10.3892/ol.2018.8345. Epub 2018 Mar 23. Oncol Lett. 2018. PMID: 29849801 Free PMC article.
-
Da Vinci robot-assisted retroperitoneal tumor resection in 105 patients: a single-center experience.Front Oncol. 2024 Jul 23;14:1414780. doi: 10.3389/fonc.2024.1414780. eCollection 2024. Front Oncol. 2024. PMID: 39109284 Free PMC article.
-
Laparoscopic liver resection-education and training.Transl Gastroenterol Hepatol. 2019 Feb 18;4:11. doi: 10.21037/tgh.2019.01.10. eCollection 2019. Transl Gastroenterol Hepatol. 2019. PMID: 30976714 Free PMC article. No abstract available.
-
Laparoscopic pancreaticoduodenectomy for periampullary tumors: lessons learned from 500 consecutive patients in a single center.Surg Endosc. 2020 Mar;34(3):1343-1352. doi: 10.1007/s00464-019-06913-9. Epub 2019 Jun 18. Surg Endosc. 2020. PMID: 31214805
References
-
- Wakabayashi G, Cherqui D, Geller DA, et al. Recommendations for laparoscopic liver resection: a report from the second international consensus conference held in Morioka. Ann Surg 2015; 261:619–629. - PubMed
-
- Dagher I, Gayet B, Tzanis D, et al. International experience for laparoscopic major liver resection. J Hepato-biliary-Pancreatic Sci 2014; 21:732–736. - PubMed
-
- Ishizawa T, Gumbs AA, Kokudo N, et al. Laparoscopic segmentectomy of the liver: from segment I to VIII. Ann Surg 2012; 256:959–964. - PubMed
-
- Honda G, Kurata M, Okuda Y, et al. Totally laparoscopic hepatectomy exposing the major vessels. J Hepatobiliary Pancreat Sci 2013; 20:435–440. - PubMed
-
- Yoon YS, Han HS, Cho JY, et al. Laparoscopic liver resection for centrally located tumors close to the hilum, major hepatic veins, or inferior vena cava. Surgery 2013; 153:502–509. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
