

Reproducibility of measurement of myometrial invasion in endometrial carcinoma
- PMID: 27787595
- PMCID: PMC5243868
- DOI: 10.1007/s00428-016-2035-5
Reproducibility of measurement of myometrial invasion in endometrial carcinoma
Abstract
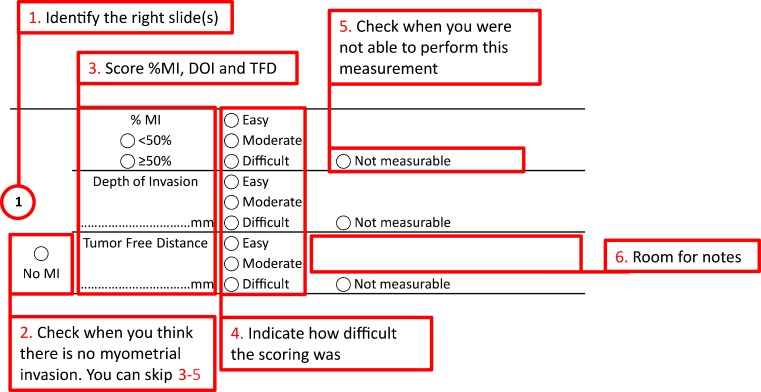
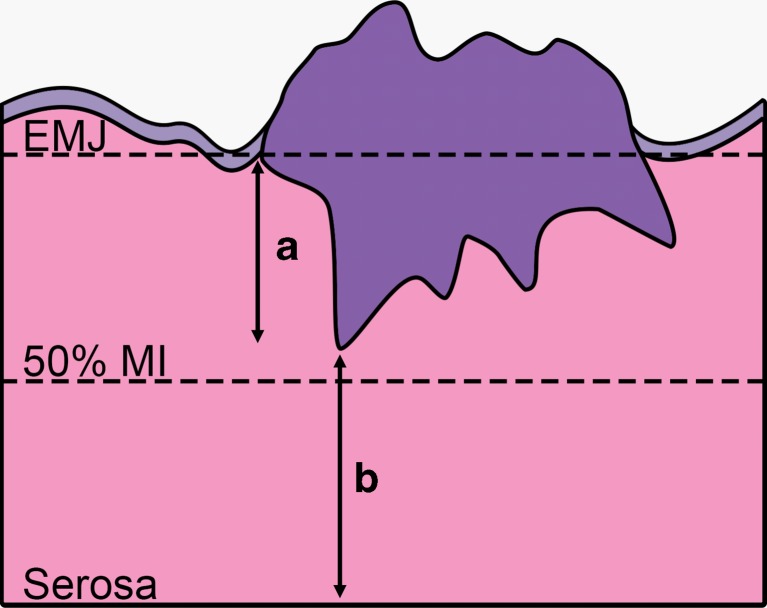
Myometrial invasion (MI) as a percentage (%MI), categorized into <50 or ≥50 %, is an important predictor of prognosis in endometrial carcinoma. Recent studies suggest that tumor-free distance (TFD) to serosa and the absolute depth of invasion (DOI) might be stronger predictors of prognosis. Although reproducibility is important in clinical practice for patient prognostication and treatment, reproducibility of these methods for the measurement of MI is largely unknown. One or two slides from 50 patients with FIGO stage I endometrioid endometrial carcinoma were viewed by seven gynecological pathologists, who were requested to measure %MI, TFD, and DOI. We categorized %MI as <50 % (including no MI) or ≥50 %, TFD as ≤1.75 or >1.75 mm (including no MI), ≤7 or >7 mm (including no MI), and ≤10 or >10 mm (including no MI) and DOI as <4 mm (including no MI) or ≥4 mm. Light's kappa for multi-rater agreement was calculated. The %MI, TFD, and DOI could be measured in 88, 83, and 79 % of cases, respectively. Kappa was 0.75 for %MI, 0.77, 0.73, and 0.69 respectively for TFD with cutoffs of 1.75, 7, and 10 mm, and 0.59 for DOI. Pathologists reach substantial agreement when measuring %MI and TFD and moderate agreement when measuring DOI. The %MI can be measured in more cases than TFD and DOI. This supports the use of %MI in daily clinical practice, but future studies should compare %MI and TFD more extensively, including inter-observer variability.
Keywords: Depth of invasion; Endometrial carcinoma; Inter-observer variability; Myometrial invasion; Tumor-free distance.
Conflict of interest statement
Compliance with ethical standards No ethical approval was needed for this study, which was performed according to the Code for Proper Secondary Use of Human Tissue (Dutch Federation of Biomedical Scientific Societies, www.federa.org). Funding This study was not funded. Conflict of interest The authors declare that they have no conflicts of interest.
Figures
References
-
- Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, Jobsen JJ, Warlam-Rodenhuis CC, De Winter KA, Lutgens LC, van den Bergh AC, van de Steen-Banasik E, Beerman H, van Lent M. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet. 2000;355(9213):1404–1411. doi: 10.1016/S0140-6736(00)02139-5. - DOI - PubMed
-
- Keys HM, Roberts JA, Brunetto VL, Zaino RJ, Spirtos NM, Bloss JD, Pearlman A, Maiman MA, Bell JG, Gynecologic Oncology G. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a gynecologic oncology group study. Gynecol Oncol. 2004;92(3):744–751. doi: 10.1016/j.ygyno.2003.11.048. - DOI - PubMed
-
- Group AES, Blake P, Swart AM, Orton J, Kitchener H, Whelan T, Lukka H, Eisenhauer E, Bacon M, Tu D, Parmar MK, Amos C, Murray C, Qian W. Adjuvant external beam radiotherapy in the treatment of endometrial cancer (MRC ASTEC and NCIC CTG EN.5 randomised trials): pooled trial results, systematic review, and meta-analysis. Lancet. 2009;373(9658):137–146. doi: 10.1016/S0140-6736(08)61767-5. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
