

Power Calculations to Select Instruments for Clinical Trial Secondary Endpoints. A Case Study of Instrument Selection for Post-Traumatic Stress Symptoms in Subjects with Acute Respiratory Distress Syndrome
- PMID: 27788018
- PMCID: PMC5291478
- DOI: 10.1513/AnnalsATS.201608-585OC
Power Calculations to Select Instruments for Clinical Trial Secondary Endpoints. A Case Study of Instrument Selection for Post-Traumatic Stress Symptoms in Subjects with Acute Respiratory Distress Syndrome
Abstract
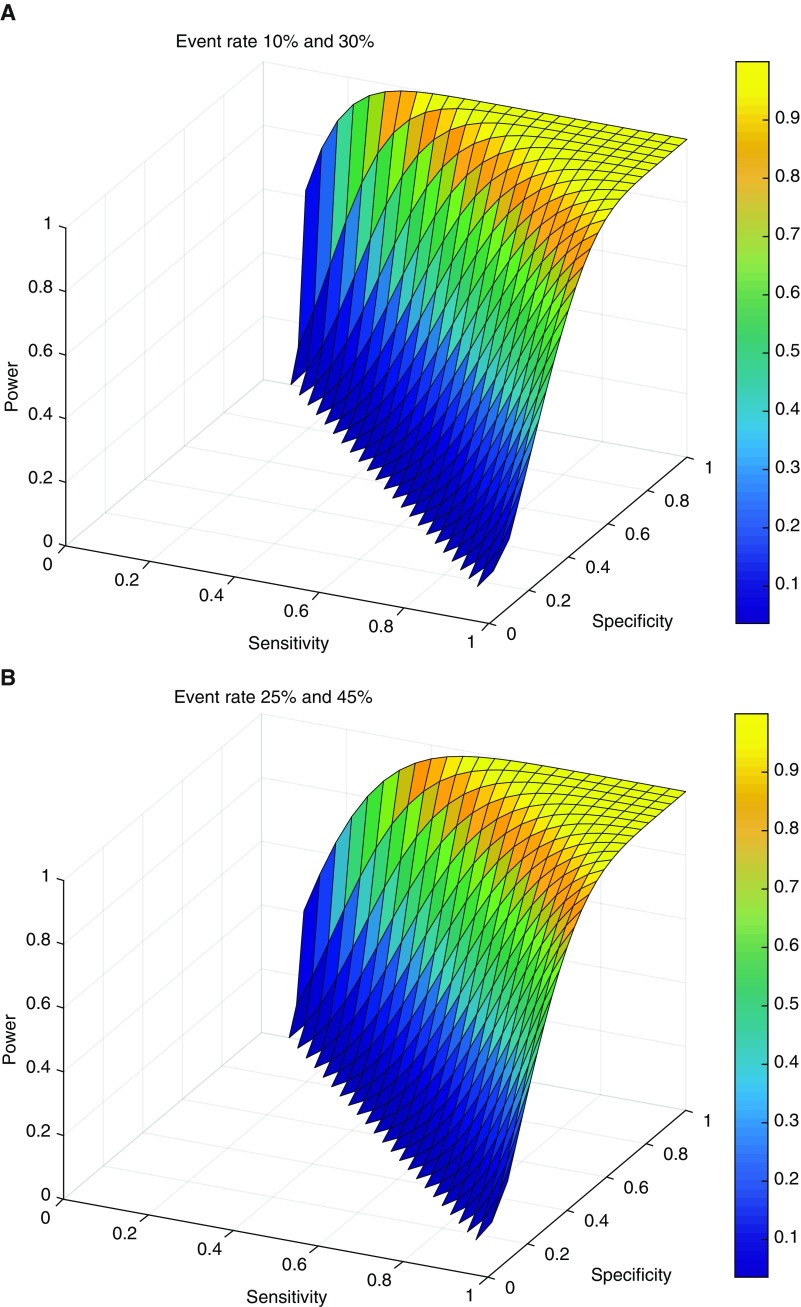
Rationale: After the sample size of a randomized clinical trial (RCT) is set by the power requirement of its primary endpoint, investigators select secondary endpoints while unable to further adjust sample size. How the sensitivity and specificity of an instrument used to measure these outcomes, together with their expected underlying event rates, affect an RCT's power to measure significant differences in these outcomes is poorly understood.
Objectives: Motivated by the design of an RCT of neuromuscular blockade in acute respiratory distress syndrome, we examined how power to detect a difference in secondary endpoints varies with the sensitivity and specificity of the instrument used to measure such outcomes.
Methods: We derived a general formula and Stata code for calculating an RCT's power to detect differences in binary outcomes when such outcomes are measured with imperfect sensitivity and specificity. The formula informed the choice of instrument for measuring post-traumatic stress-like symptoms in the Reevaluation of Systemic Early Neuromuscular Blockade RCT ( www.clinicaltrials.gov identifier NCT02509078).
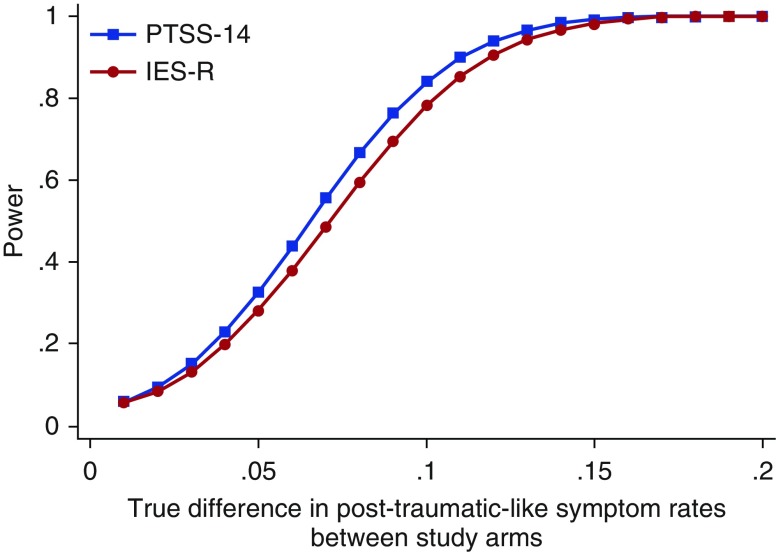
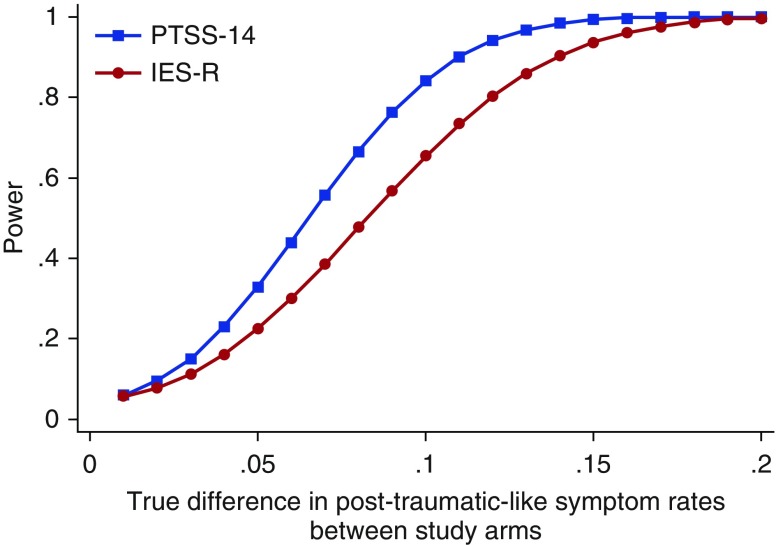
Measurements and main results: On the basis of published sensitivities and specificities, the Impact of Events Scale-Revised was predicted to measure a 36% symptom rate, whereas the Post-Traumatic Stress Symptoms instrument was predicted to measure a 23% rate, if the true underlying rate of post-traumatic stress symptoms were 25%. Despite its lower sensitivity, the briefer Post-Traumatic Stress Symptoms instrument provided superior power to detect a difference in rates between trial arms, owing to its higher specificity.
Conclusions: Examining instruments' power to detect differences in outcomes may guide their selection when multiple instruments exist, each with different sensitivities and specificities.
Keywords: bias; clinical trials; critical care outcomes; sensitivity; specificity.
Figures

Comment in
-
Reply: Validity of the Posttraumatic Stress Symptoms-14 Instrument in Acute Respiratory Failure Survivors.Ann Am Thorac Soc. 2017 Jun;14(6):1048-1049. doi: 10.1513/AnnalsATS.201703-195LE. Ann Am Thorac Soc. 2017. PMID: 28355087 Free PMC article. No abstract available.
-
Validity of the Posttraumatic Stress Symptoms-14 Instrument in Acute Respiratory Failure Survivors.Ann Am Thorac Soc. 2017 Jun;14(6):1047-1048. doi: 10.1513/AnnalsATS.201702-112LE. Ann Am Thorac Soc. 2017. PMID: 28355099 Free PMC article. No abstract available.
References
-
- ClincialTrials.gov. Reevaluation of Systemic Early Neuromuscular Blockade (ROSE) [accessed 2015 Dec 1]. Available from: https://clinicaltrials.gov/ct2/show/NCT02509078.
-
- Twigg E, Humphris G, Jones C, Bramwell R, Griffiths RD. Use of a screening questionnaire for post-traumatic stress disorder (PTSD) on a sample of UK ICU patients. Acta Anaesthesiol Scand. 2008;52:202–208. - PubMed
-
- Stoll C, Kapfhammer HP, Rothenhäusler HB, Haller M, Briegel J, Schmidt M, Krauseneck T, Durst K, Schelling G. Sensitivity and specificity of a screening test to document traumatic experiences and to diagnose post-traumatic stress disorder in ARDS patients after intensive care treatment. Intensive Care Med. 1999;25:697–704. - PubMed
-
- Jones C, Bäckman C, Capuzzo M, Flaatten H, Rylander C, Griffiths RD. Precipitants of post-traumatic stress disorder following intensive care: a hypothesis generating study of diversity in care. Intensive Care Med. 2007;33:978–985. - PubMed
MeSH terms
Substances
Associated data
Grants and funding
- U01 HL123031/HL/NHLBI NIH HHS/United States
- U01 HL123020/HL/NHLBI NIH HHS/United States
- U01 HL122989/HL/NHLBI NIH HHS/United States
- U01 HL123009/HL/NHLBI NIH HHS/United States
- K24 HL089223/HL/NHLBI NIH HHS/United States
- U01 HL123004/HL/NHLBI NIH HHS/United States
- U01 HL123008/HL/NHLBI NIH HHS/United States
- U01 HL123022/HL/NHLBI NIH HHS/United States
- U01 HL123023/HL/NHLBI NIH HHS/United States
- U01 HL123027/HL/NHLBI NIH HHS/United States
- U01 HL122998/HL/NHLBI NIH HHS/United States
- T32 HL007749/HL/NHLBI NIH HHS/United States
- U01 HL123018/HL/NHLBI NIH HHS/United States
- U01 HL123033/HL/NHLBI NIH HHS/United States
- U01 HL123010/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
