

Progressive Decline of Lung Function in Rheumatoid Arthritis-Associated Interstitial Lung Disease
- PMID: 27788297
- PMCID: PMC5328843
- DOI: 10.1002/art.39971
Progressive Decline of Lung Function in Rheumatoid Arthritis-Associated Interstitial Lung Disease
Abstract
Objective: Interstitial lung disease (ILD) is associated with substantial morbidity in rheumatoid arthritis (RA), but very little is known about its long-term progression. This study was undertaken to investigate the progression of pulmonary disease using a large single-center cohort of patients with RA-associated ILD.
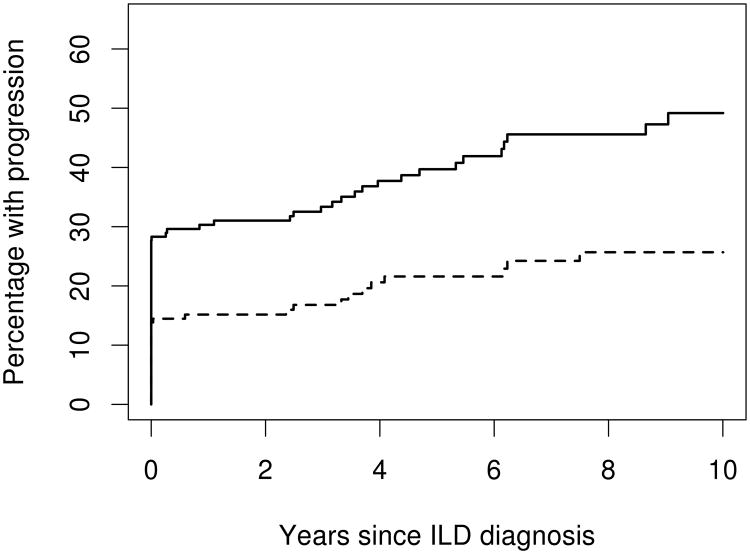
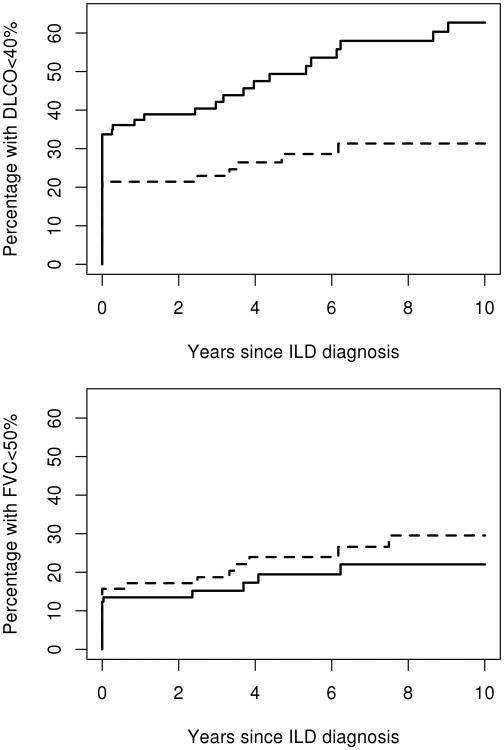
Methods: Records of all patients with RA-associated ILD seen at Mayo Clinic between 1998 and 2014, with at least 4 weeks follow-up and at least 1 pulmonary function test, were identified and manually screened for study inclusion. Progression was defined as a diffusing capacity for carbon monoxide (DLco) <40% predicted (or patients whose illness was too advanced to undergo screening) or a forced vital capacity (FVC) <50% predicted. Time to progression was analyzed using the Kaplan-Meier method.
Results: Of the 167 patients included in the study, 81 (49%) were female, with a mean ± SD age of 67 ± 10 years at diagnosis of ILD. Median follow-up time from diagnosis of ILD was 3.3 years (range 0.01-14.8). One-third of the patients required supplemental oxygen, 40% developed DLco <40% predicted, and 22% developed FVC <50% predicted within 5 years after ILD diagnosis. Usual interstitial pneumonia (UIP) versus nonspecific interstitial pneumonia (NSIP) was a risk factor for DLco progression (hazard ratio 3.29 [95% confidence interval 1.28-8.41]). Lower DLco and FVC at baseline increased the risk for progression to DLco <40% predicted and FVC <50% predicted, and higher rates of change in the first 6 months also increased the risk of progression.
Conclusion: Progressive loss of pulmonary function is common in RA-associated ILD and is worse in patients with UIP than in those with NSIP. Predictors of progression in patients with RA-associated ILD may aid clinicians in identifying patients at highest risk for progression of ILD.
© 2016, American College of Rheumatology.
Conflict of interest statement
Conflict of interest: The authors have no relevant conflicts of interest to disclose
Figures
References
-
- Suzuki A, Ohosone Y, Obana M, Mita S, Matsuoka Y, Irimajiri S, et al. Cause of death in 81 autopsied patients with rheumatoid arthritis. J Rheumatol. 1994;21(1):33–6. - PubMed
-
- Doyle JJ, Eliasson AH, Argyros GJ, Dennis GJ, Finger DR, Hurwitz KM, et al. Prevalence of pulmonary disorders in patients with newly diagnosed rheumatoid arthritis. Clin Rheumatol. 2000;19(3):217–21. - PubMed
-
- Travis WD, Costabel U, Hansell DM, King TE, Jr, Lynch DA, Nicholson AG, et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–48. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
