

Intracranial Arteriovenous Shunting: Detection with Arterial Spin-Labeling and Susceptibility-Weighted Imaging Combined
- PMID: 27789452
- PMCID: PMC7963679
- DOI: 10.3174/ajnr.A4961
Intracranial Arteriovenous Shunting: Detection with Arterial Spin-Labeling and Susceptibility-Weighted Imaging Combined
Abstract
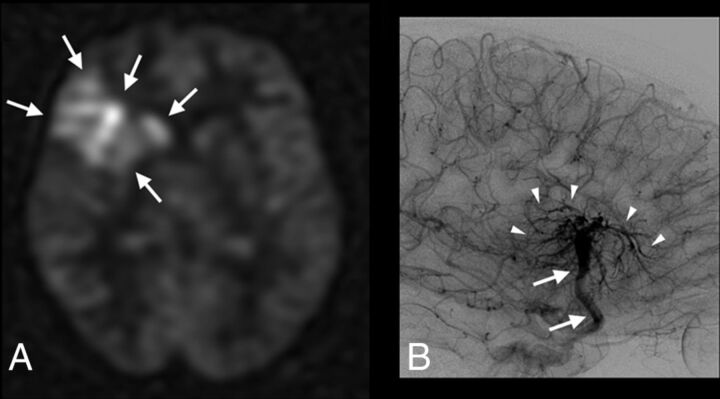
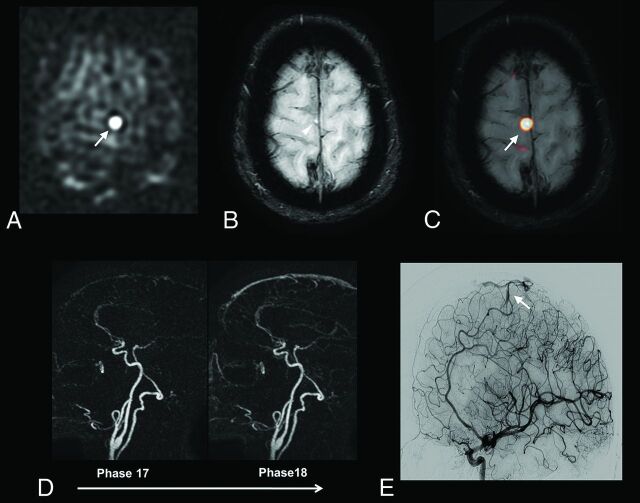
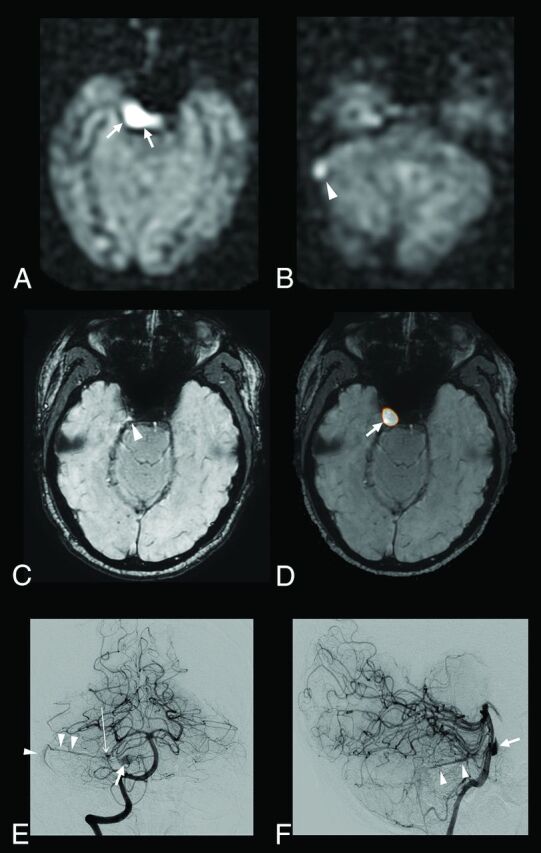
Background and purpose: Arterial spin-labeling and susceptibility-weighted imaging are 2 MR imaging techniques that do not require gadolinium. The study aimed to assess the accuracy of arterial spin-labeling and SWI combined for detecting intracranial arteriovenous shunting in comparison with conventional MR imaging.
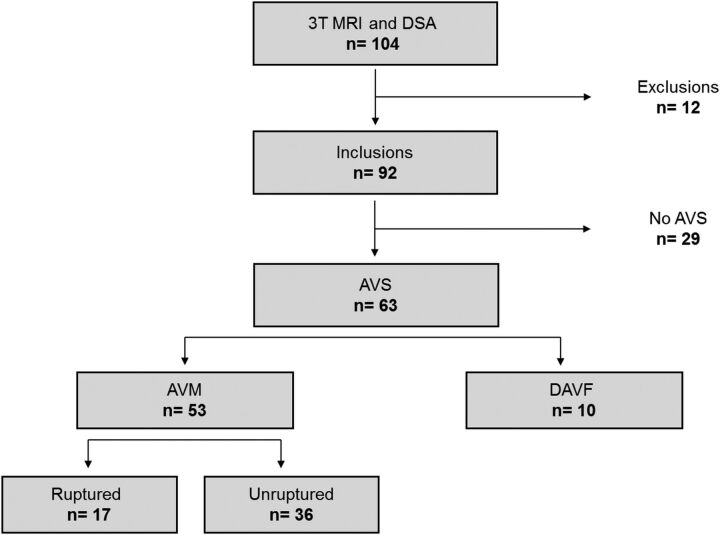
Materials and methods: Ninety-two consecutive patients with a known (n = 24) or suspected arteriovenous shunting (n = 68) underwent digital subtraction angiography and brain MR imaging, including arterial spin-labeling/SWI and conventional angiographic MR imaging (3D TOF, 4D time-resolved, and 3D contrast-enhanced MRA). Arterial spin-labeling/SWI and conventional MR imaging were reviewed separately in a randomized order by 2 blinded radiologists who judged the presence or absence of arteriovenous shunting. The accuracy of arterial spin-labeling/SWI for the detection of arteriovenous shunting was calculated by using the area under receiver operating curve with DSA as reference standard. κ coefficients were computed to determine interobserver and intermodality agreement.
Results: Of the 92 patients, DSA showed arteriovenous shunting in 63 (arteriovenous malformation in 53 and dural arteriovenous fistula in 10). Interobserver agreement was excellent (κ =0.83-0.95). In 5 patients, arterial spin-labeling/SWI correctly detected arteriovenous shunting, while the conventional angiographic MR imaging did not. Compared with conventional MR imaging, arterial spin-labeling/SWI was significantly more sensitive (0.98 versus 0.90, P = .04) and equally specific (0.97) and showed significantly higher agreement with DSA (κ = 0.95 versus 0.84, P = .01) and higher area under the receiver operating curve (0.97 versus 0.93, P = .02).
Conclusions: Our study showed that the combined use of arterial spin-labeling and SWI may be an alternative to contrast-enhanced MRA for the detection of intracranial arteriovenous shunting.
© 2017 by American Journal of Neuroradiology.
Figures
Comment in
-
Reply.AJNR Am J Neuroradiol. 2017 May;38(5):E33. doi: 10.3174/ajnr.A5131. Epub 2017 Feb 23. AJNR Am J Neuroradiol. 2017. PMID: 28232498 Free PMC article. No abstract available.
-
Intracranial Arteriovenous Shunting Detection with Arterial Spin-Labeling and Susceptibility-Weighted Imaging: Potential Pitfall of a Venous Predominant Parenchymal Arteriovenous Malformation.AJNR Am J Neuroradiol. 2017 May;38(5):E32. doi: 10.3174/ajnr.A5108. Epub 2017 Feb 23. AJNR Am J Neuroradiol. 2017. PMID: 28232499 Free PMC article. No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical