

Prognostic Effect of Isolated Nocturnal Hypertension in Chinese Patients With Nondialysis Chronic Kidney Disease
- PMID: 27792646
- PMCID: PMC5121515
- DOI: 10.1161/JAHA.116.004198
Prognostic Effect of Isolated Nocturnal Hypertension in Chinese Patients With Nondialysis Chronic Kidney Disease
Abstract
Background: Isolated nocturnal hypertension (INH) has been studied among the general population and hypertensive patients. However, little insight is available on the prognostic effect of INH in patients with chronic kidney disease (CKD). This study investigated the prognostic effect of INH in a cohort of Chinese patients with nondialysis CKD.
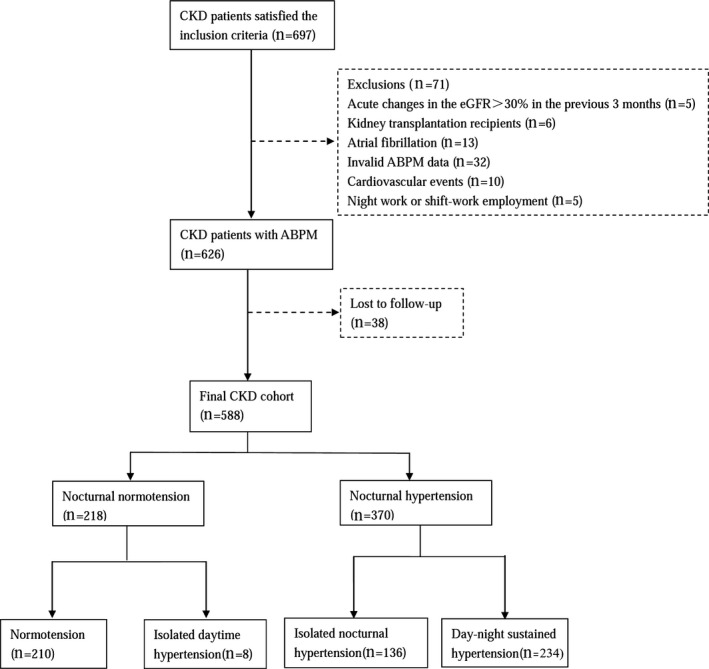
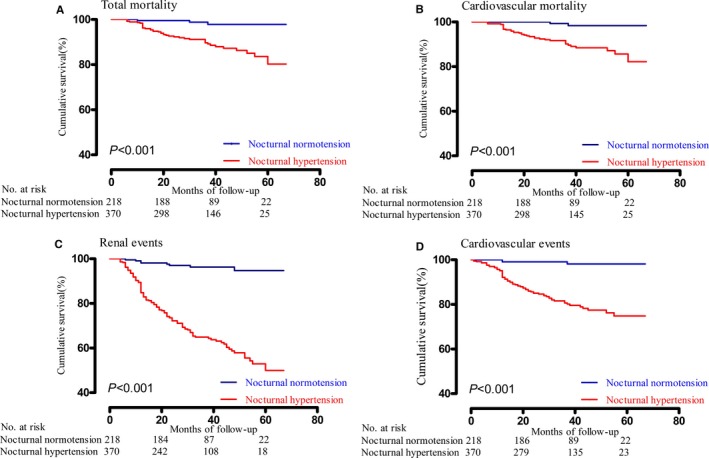
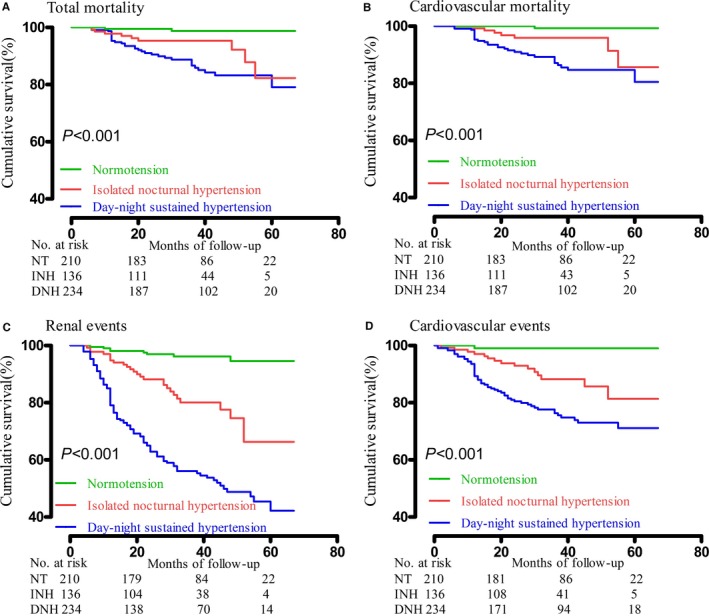
Methods and results: A total of 588 Chinese CKD patients who were admitted to the Third Affiliated Hospital of Sun Yat-Sen University were enrolled in this study. We monitored blood pressure (BP) throughout the day and followed health outcomes in the 588 CKD patients admitted to our hospital division. We recorded time to total mortality, cardiovascular mortality, renal events, and cardiovascular events. A total of 370 (62.92%) individuals had nocturnal hypertension, which included 136 (23.13%) patients with INH. Multivariable Cox regression analyses showed that nocturnal BP was a significant risk factor for renal events and cardiovascular events in CKD patients, even when adjusted for clinic BP, 24-hour BP, or daytime BP. Patients with nocturnal hypertension showed a worse prognosis compared with patients with nocturnal normotension (P<0.05), and nocturnal hypertension (versus nocturnal normotension) was associated with an increased risk for renal events (hazard ratio [HR], 3.81; 95% CI, 1.74-8.36) and cardiovascular events (HR, 8.34; 95% CI, 1.98-35.07). In addition, patients with INH had a worse prognosis than patients with normotension (P<0.017), whereas INH (versus normotension) was associated with a higher risk of renal events (HR, 2.78; 95% CI, 1.16-6.65) and cardiovascular events (HR, 6.82; 95% CI, 1.52-30.63).
Conclusions: INH was associated with a poor prognosis in Chinese nondialysis CKD patients.
Keywords: ambulatory blood pressure monitoring; chronic kidney disease; hypertension; isolated nocturnal hypertension; kidney; kidney (diabetes); prognosis.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Similar articles
-
High prevalence of isolated nocturnal hypertension in Chinese patients with chronic kidney disease.J Am Heart Assoc. 2015 Jun 18;4(6):e002025. doi: 10.1161/JAHA.115.002025. J Am Heart Assoc. 2015. PMID: 26089178 Free PMC article.
-
Prognostic value of nighttime blood pressure load in Chinese patients with nondialysis chronic kidney disease.J Clin Hypertens (Greenwich). 2017 Sep;19(9):890-898. doi: 10.1111/jch.13017. Epub 2017 May 7. J Clin Hypertens (Greenwich). 2017. PMID: 28480628 Free PMC article.
-
Dipping Status, Ambulatory Blood Pressure Control, Cardiovascular Disease, and Kidney Disease Progression: A Multicenter Cohort Study of CKD.Am J Kidney Dis. 2023 Jan;81(1):15-24.e1. doi: 10.1053/j.ajkd.2022.04.010. Epub 2022 Jun 13. Am J Kidney Dis. 2023. PMID: 35709922
-
Prognostic Effect of the Nocturnal Blood Pressure Fall in Hypertensive Patients: The Ambulatory Blood Pressure Collaboration in Patients With Hypertension (ABC-H) Meta-Analysis.Hypertension. 2016 Apr;67(4):693-700. doi: 10.1161/HYPERTENSIONAHA.115.06981. Epub 2016 Feb 22. Hypertension. 2016. PMID: 26902495 Review.
-
Sleep-time blood pressure: Unique sensitive prognostic marker of vascular risk and therapeutic target for prevention.Sleep Med Rev. 2017 Jun;33:17-27. doi: 10.1016/j.smrv.2016.04.001. Epub 2016 Apr 14. Sleep Med Rev. 2017. PMID: 27316324 Review.
Cited by
-
Hypertension in China: epidemiology and treatment initiatives.Nat Rev Cardiol. 2023 Aug;20(8):531-545. doi: 10.1038/s41569-022-00829-z. Epub 2023 Jan 11. Nat Rev Cardiol. 2023. PMID: 36631532 Review.
-
Isolated nocturnal hypertension in relation to host and environmental factors and clock genes.J Clin Hypertens (Greenwich). 2022 Oct;24(10):1255-1262. doi: 10.1111/jch.14532. Epub 2022 Aug 9. J Clin Hypertens (Greenwich). 2022. PMID: 35942908 Free PMC article.
-
The association of SBP with mortality in patients with stage 1-4 chronic kidney disease.J Hypertens. 2021 Nov 1;39(11):2250-2257. doi: 10.1097/HJH.0000000000002927. J Hypertens. 2021. PMID: 34232158 Free PMC article.
-
Circadian blood pressure variability and associated factors among chronic kidney disease patients at Nekemte Town public Hospitals, West Oromia, Ethiopia: a comparative cross-sectional study.BMJ Open. 2024 Aug 28;14(8):e083014. doi: 10.1136/bmjopen-2023-083014. BMJ Open. 2024. PMID: 39209493 Free PMC article.
-
Prevalence and characteristics of isolated nocturnal hypertension in the general population.Korean J Intern Med. 2021 Sep;36(5):1126-1133. doi: 10.3904/kjim.2021.022. Epub 2021 Apr 5. Korean J Intern Med. 2021. PMID: 34503319 Free PMC article.
References
-
- Stenvinkel P. Chronic kidney disease: a public health priority and harbinger of premature cardiovascular disease. J Intern Med. 2010;268:456–467. - PubMed
-
- Zhang L, Wang F, Wang L, Wang W, Liu B, Liu J, Chen M, He Q, Liao Y, Yu X, Chen N, Zhang JE, Hu Z, Liu F, Hong D, Ma L, Liu H, Zhou X, Chen J, Pan L, Chen W, Wang W, Li X, Wang H. Prevalence of chronic kidney disease in China: a cross‐sectional survey. Lancet. 2012;379:815–822. - PubMed
-
- The Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration Writing and global analysis group . Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol. 2014;2:634–647. - PMC - PubMed
-
- Johnson ES, Thorp ML, Yang X, Charansonney OL, Smith DH. Predicting renal replacement therapy and mortality in CKD. Am J Kidney Dis. 2007;50:559–565. - PubMed
-
- Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, McAlister F, Garg AX. Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol. 2006;17:2034–2047. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
