

Treatment Intensification for Hypertension in US Ambulatory Medical Care
- PMID: 27792661
- PMCID: PMC5121514
- DOI: 10.1161/JAHA.116.004188
Treatment Intensification for Hypertension in US Ambulatory Medical Care
Abstract
Background: Hypertension is widely prevalent yet remains uncontrolled in nearly half of US hypertensive adults. Treatment intensification for hypertension reduces rates of major cardiovascular events and all-cause mortality, but clinical inertia remains a notable impediment to further improving hypertension control. This study examines the likelihood and determinants of treatment intensification with new medication in US ambulatory medical care.
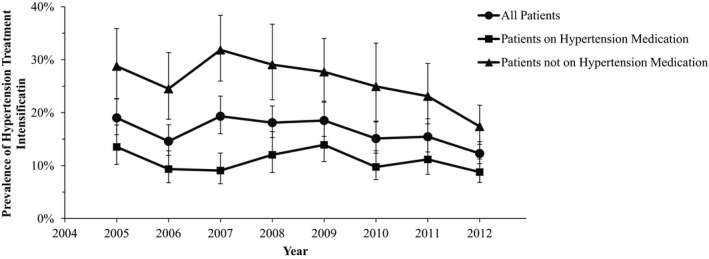
Methods and results: Using the nationally representative National Ambulatory Medical Care Survey (2005-2012) and National Hospital Ambulatory Medical Care Survey (2005-2011), we identified adult primary care visits with diagnosed hypertension and documented blood pressure exceeding goal targets and assessed the weighted prevalence and odds ratios of treatment intensification by initiation or addition of new medication. Approximately 41.7 million yearly primary care visits (crude N: 14 064, 2005-2012) occurred among US hypertensive adults with documented blood pressure ≥140/90 mm Hg, where treatment intensification may be beneficial. However, only 7.0 million of these visits (95% confidence interval 6.2-7.8 million) received treatment intensification with new medication, a weighted prevalence of 16.8% (15.8% to 17.9%). This proportion was consistently low and decreased over time. This decline was largely driven by decreasing medication initiation levels among patients on no previous hypertension medications from 31.8% (26.0% to 38.4%) in 2007 to 17.4% (14.0% to 21.4%) in 2012, while medication addition levels remained more stable over time.
Conclusions: US hypertensive adults received treatment intensification with new medication in only 1 out of 6 primary care visits, a fraction that is declining over time. A profound increase in intensification remains a vast opportunity to maximally reduce hypertension-related morbidity and mortality nationwide.
Keywords: blood pressure; hypertension medication; medication addition; medication initiation.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Comment in
-
Hypertension Management: Ripe for Disruption.J Am Heart Assoc. 2016 Oct 22;5(10):e004681. doi: 10.1161/JAHA.116.004681. J Am Heart Assoc. 2016. PMID: 27792663 Free PMC article. No abstract available.
References
-
- Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS data brief, no 133. Hyattsville, MD: National Center for Health Statistics. 2013. - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Després J‐P, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB; on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:e29–e322. - PubMed
-
- James PA, Oparil S, Carter BL, Cushman WC, Dennison‐Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E. 2014 evidence‐based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–520. - PubMed
-
- Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
