

Impact of diabetes mellitus on risk of cardiovascular disease and all-cause mortality: Evidence on health outcomes and antidiabetic treatment in United States adults
- PMID: 27795819
- PMCID: PMC5065665
- DOI: 10.4239/wjd.v7.i18.449
Impact of diabetes mellitus on risk of cardiovascular disease and all-cause mortality: Evidence on health outcomes and antidiabetic treatment in United States adults
Abstract
Aim: To examine the epidemic of diabetes mellitus (DM) and its impact on mortality from all-cause and cardiovascular disease (CVD), and to test the effect of antidiabetic therapy on the mortality in United States adults.
Methods: The analysis included a randomized population sample of 272149 subjects ages ≥ 18 years who participated in the National Health Interview Surveys (NHIS) in 2000-2009. Chronic conditions (hypertension, DM and CVD) were classified by participants' self-reports of physician diagnosis. NHIS-Mortality Linked Files, and NHIS-Medical Expenditure Panel Survey Linkage Files on prescribed medicines for patients with DM were used to test the research questions. χ2, Poisson and Cox's regression models were applied in data analysis.
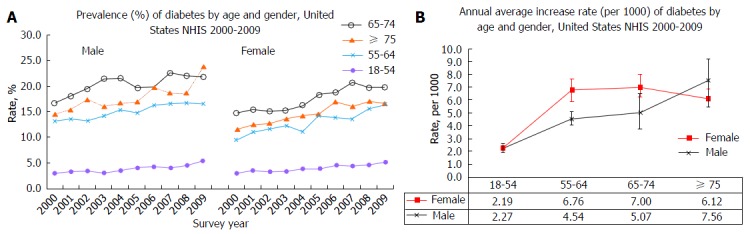
Results: Of all participants, 22305 (8.2%) had DM. The prevalence of DM significantly increased from 2000 to 2009 in all age groups (P < 0.001). Within an average 7.39 (SD = 3) years of follow-up, male DM patients had 1.56 times higher risk of death from all-cause (HR = 1.56, 95%CI: 1.49-1.64), 1.72 times higher from heart disease [1.72 (1.53-1.93)], 1.48 times higher from cerebrovascular disease [1.48 (1.18-1.85)], and 1.67 times higher from CVD [1.67 (1.51-1.86)] than subjects without DM, respectively. Similar results were observed in females. In males, 10% of DM patients did not use any antidiabetic medications, 38.1% used antidiabetic monotherapy, and 51.9% used ≥ 2 antidiabetic medications. These corresponding values were 10.3%, 40.4% and 49.4% in females. A significant protective effect of metformin monotherapy or combination therapy (except for insulin) on all-cause mortality and a protective but non-significant effect on CVD mortality were observed.
Conclusion: This is the first study using data from multiple linkage files to confirm a significant increased prevalence of DM in the last decade in the United States. Patients with DM have significantly higher risk of death from all-cause and CVD than those without DM. Antidiabetic mediations, specifically for metformin use, show a protective effect against all-cause and CVD mortalities.
Keywords: Cardiovascular disease; Epidemic of diabetes mellitus; Pharmacoepidemiologic profiles; United States.
Conflict of interest statement
Conflict-of-interest statement: We have no conflict of interest to report.
Figures



References
-
- Association AD. Statistics About Diabetes. [accessed 2014 Jan 15] Available from: http://www.diabetes.org/diabetes-basics/statistics/
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–1053. - PubMed
-
- Liu L, Yin X, Morrissey S. Global variability in diabetes mellitus and its association with body weight and primary healthcare support in 49 low- and middle-income developing countries. Diabet Med. 2012;29:995–1002. - PubMed
-
- Meetoo D, McGovern P, Safadi R. An epidemiological overview of diabetes across the world. Br J Nurs. 2007;16:1002–1007. - PubMed
-
- Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002;287:2570–2581. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
