

National trends in inpatient admissions following stereotactic radiosurgery and the in-hospital patient outcomes in the United States from 1998 to 2011
- PMID: 27795870
- PMCID: PMC5081223
National trends in inpatient admissions following stereotactic radiosurgery and the in-hospital patient outcomes in the United States from 1998 to 2011
Abstract
Purpose: This study sought to examine trends in stereotactic radiosurgery (SRS) and in-hospital patient outcomes on a national level by utilizing national administrative data from the Nationwide Inpatient Sample (NIS) database.
Methods and materials: Using the NIS database, all discharges where patients underwent inpatient SRS were included in our study from 1998 - 2011 as designated by the ICD9-CM procedural codes. Trends in the utilization of primary and adjuvant SRS, in-hospital complications and mortality, and resource utilization were identified and analyzed.
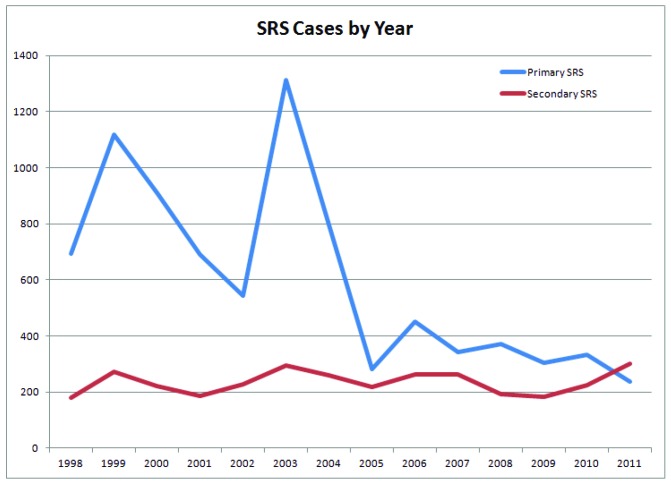
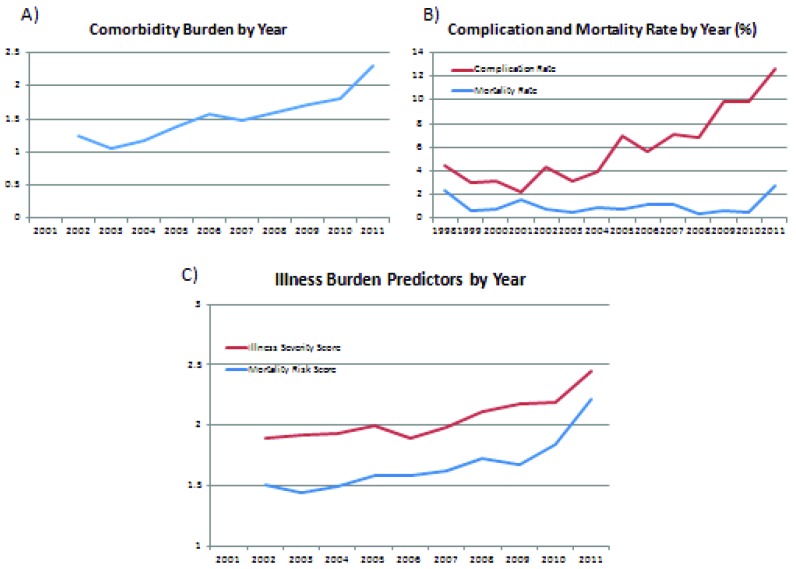
Results: Our study included over 11,000 hospital discharges following admission for primary SRS or for adjuvant SRS following admission for surgery or other indication. The most popular indication for SRS continues to be treatment of intracranial metastatic disease (36.7%), but expansion to primary CNS lesions and other non-malignant pathology beyond trigeminal neuralgia has occurred over the past decade. Second, inpatient admissions for primary SRS have declined by 65.9% over this same period of time. Finally, as inpatient admissions for SRS become less frequent, the complexity and severity of illness seen in admitted patients has increased over time with an increase in the average comorbidity score from 1.25 in the year 2002 to 2.29 in 2011, and an increase in over-all in-hospital complication rate of 2.8 times over the entire study period.
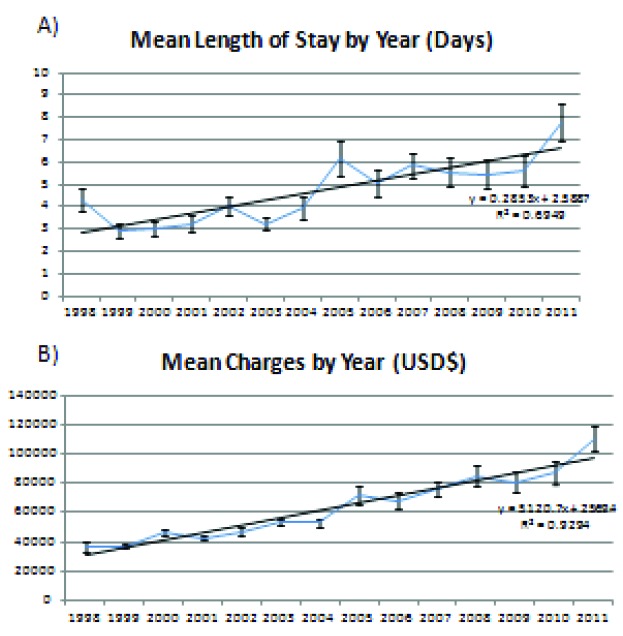
Conclusions: As the practice of SRS continues to evolve, we have seen several trends in associated hospital admissions. Overall, the number of inpatient admissions for primary SRS has declined while adjuvant applications have remained stable. Over the same period, there has been associated increase in complication rate, length of stay, and mortality in inpatients. These associations may be explained by an increase in the comorbidity-load of admitted patients as more high-risk patients are selected for admission at inpatient centers while more stable patients are increasingly being referred to outpatient centers.
Keywords: Nationwide Inpatient Sample; complications; mortality; radiosurgery outcomes; stereotactic radiosurgery; usage trends.
Conflict of interest statement
Authors’ disclosure of potential conflicts of interest Dr. Allen Ho and Alexander Li are members of and received grants from the Stanford Society of Physician Scholars which were utilized during the conduct of the study. This research was supported by the Office of the Dean, Stanford School of Medicine. This work was supported in part by the Stanford Clinical and Translational Science Award (CTSA) to Spectrum (UL1 TR001085). The CTSA program is led by the National Center for Advancing Translational Sciences (NCATS) at the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Figures
Similar articles
-
Limitations of using population-based databases to assess trends in spinal stereotactic radiosurgery.J Radiosurg SBRT. 2016;4(3):177-180. J Radiosurg SBRT. 2016. PMID: 29296442 Free PMC article.
-
Trends in surgical treatment for trigeminal neuralgia in the United States of America from 1988 to 2008.J Clin Neurosci. 2013 Nov;20(11):1538-45. doi: 10.1016/j.jocn.2012.12.026. Epub 2013 Aug 7. J Clin Neurosci. 2013. PMID: 23932422
-
Trends in the surgical treatment for spinal metastasis and the in-hospital patient outcomes in the United States from 2000 to 2009.Spine J. 2014 Sep 1;14(9):1844-9. doi: 10.1016/j.spinee.2013.11.029. Epub 2013 Nov 27. Spine J. 2014. PMID: 24291034
-
Stereotactic radiosurgery versus stereotactic radiotherapy in the management of intracranial meningiomas: a systematic review and meta-analysis.Neurosurg Focus. 2019 Jun 1;46(6):E2. doi: 10.3171/2019.3.FOCUS1970. Neurosurg Focus. 2019. PMID: 31153149
-
Clinical Research Using the National Inpatient Sample: A Brief Review of Colorectal Studies Utilizing the NIS Database.Clin Colon Rectal Surg. 2019 Jan;32(1):33-40. doi: 10.1055/s-0038-1673352. Epub 2019 Jan 8. Clin Colon Rectal Surg. 2019. PMID: 30647544 Free PMC article. Review.
Cited by
-
Gyroscopic Stereotactic Radiosurgery: A Retrospective Analysis.Cureus. 2025 Jul 22;17(7):e88553. doi: 10.7759/cureus.88553. eCollection 2025 Jul. Cureus. 2025. PMID: 40851739 Free PMC article.
-
The evolution of stereotactic radiosurgery in neurosurgical practice.J Neurooncol. 2021 Feb;151(3):451-459. doi: 10.1007/s11060-020-03392-0. Epub 2021 Feb 21. J Neurooncol. 2021. PMID: 33611711 Review.
-
Readmission following inpatient stereotactic radiosurgery for brain tumors.J Radiosurg SBRT. 2019;6(2):101-119. J Radiosurg SBRT. 2019. PMID: 31641547 Free PMC article.
-
Hospitalization outcomes among brain metastasis patients receiving radiation therapy with or without stereotactic radiosurgery from the 2005-2014 Nationwide Inpatient Sample.Sci Rep. 2021 Sep 28;11(1):19209. doi: 10.1038/s41598-021-98563-y. Sci Rep. 2021. PMID: 34584139 Free PMC article.
References
-
- Leksell L. The stereotaxic method and radiosurgery of the brain. Acta chirurgica Scandinavica 1951;102:316-319. - PubMed
-
- Lunsford LD, Maitz A, Lindner G. First united states 201 source cobalt-60 gamma unit for radiosurgery. Applied neurophysiology 1987;50:253-256. - PubMed
-
- Barnett GH, Linskey ME, Adler JR, Cozzens JW, Friedman WA, Heilbrun MP, Lunsford LD, Schulder M, Sloan AE, American Association of Neurological S. Congress of Neurological Surgeons Washington Committee Stereotactic Radiosurgery Task F Stereotactic radiosurgery--an organized neurosurgery-sanctioned definition. Journal of neurosurgery 2007;106:1-5. - PubMed
-
- Pannullo SC, Fraser JF, Moliterno J, Cobb W, Stieg PE. Stereotactic radiosurgery: A meta-analysis of current therapeutic applications in neuro-oncologic disease. J Neurooncol 2011;103:1-17. - PubMed
-
- Kooy HM, Nedzi LA, Loeffler JS, Alexander E, 3rd, Cheng CW, Mannarino EG, Holupka EJ, Siddon RL. Treatment planning for stereotactic radiosurgery of intra-cranial lesions. International journal of radiation oncology, biology, physics 1991;21:683-693. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous