

Healthcare Fragmentation and the Frequency of Radiology and Other Diagnostic Tests: A Cross-Sectional Study
- PMID: 27796694
- PMCID: PMC5264678
- DOI: 10.1007/s11606-016-3883-z
Healthcare Fragmentation and the Frequency of Radiology and Other Diagnostic Tests: A Cross-Sectional Study
Abstract
Background: Fragmented ambulatory care has been associated with high rates of emergency department visits and hospitalizations, but effects on other types of utilization are unclear.
Objective: To determine whether more fragmented care is associated with more radiology and other diagnostic tests, compared to less fragmented care.
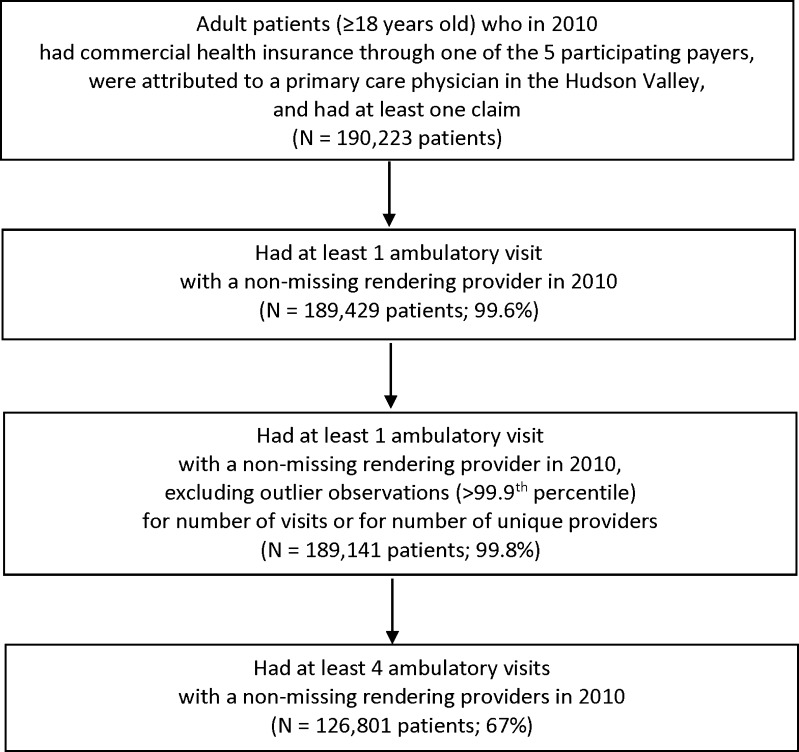
Design: We conducted a cross-sectional study using claims from five commercial payers for 2010. The study took place in the Hudson Valley, a seven-county region in New York State.
Participants: We included adult patients who were insured through the participating payers and were attributed to a primary care physician in the region. We restricted the cohort to those with ≥4 ambulatory visits, as measures of fragmentation are not reliable if based on ≤3 visits (N = 126,801).
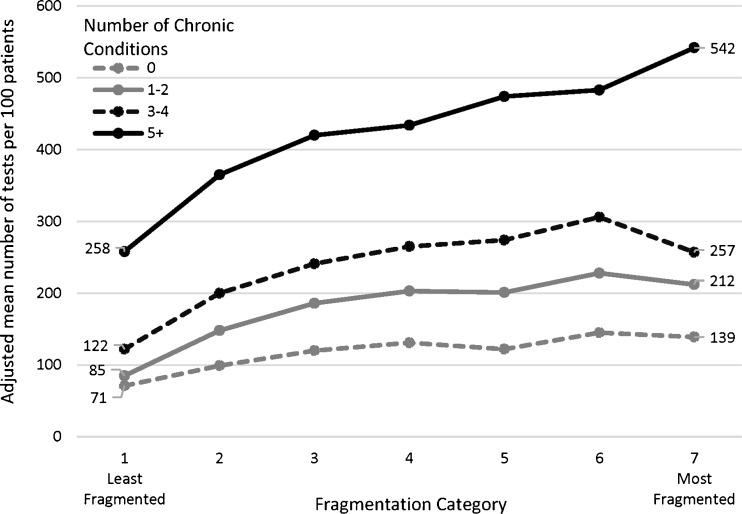
Main measures: For each patient, we calculated fragmentation using a reversed Bice-Boxerman Index, which we divided into seven categories. We used negative binomial regression to determine the association between fragmentation category and rates of radiology and other diagnostic tests, stratified by number of chronic conditions and adjusting for patient age, gender, and number of visits.
Key results: Patients with the most fragmented care had approximately twice as many radiology and other diagnostic tests as patients with the least fragmented care, across all groups stratified by number of chronic conditions (each adjusted p < 0.0001). For example, among patients with ≥5 chronic conditions, those with the least fragmented care had 258 tests per 100 patients, and those with the most fragmented care had 542 tests per 100 patients (+284 tests per 100 patients, or +110 %, adjusted p < 0.0001).
Conclusion: More fragmented care was independently associated with higher rates of radiology and other diagnostic tests than less fragmented care.
Keywords: ambulatory care; healthcare utilization; radiology.
Conflict of interest statement
Compliance with Ethical Standards Institutional review boards at Weill Cornell Medical College and Kingston Hospital approved the protocol. Conflict of Interest The authors declare that they do not have a conflict of interest. Funders This study was funded by the Commonwealth Fund (grant #20140960), which supported efforts by Dr. Kern and Ms. Seirup. The funding source had no role in the study design, conduct, or reporting. Dr. Kern and Ms. Seirup had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Presentations This work was presented at the national meeting of the Society of General Internal Medicine on May 13, 2016.
Figures
Comment in
-
Capsule Commentary on Kern et al., Healthcare Fragmentation and the Frequency of Radiology and Other Diagnostic Tests: a Cross-Sectional Study.J Gen Intern Med. 2017 Feb;32(2):190. doi: 10.1007/s11606-016-3953-2. J Gen Intern Med. 2017. PMID: 27957664 Free PMC article. No abstract available.
References
-
- Liu CW, Einstadter D, Cebul RD. Care fragmentation and emergency department use among complex patients with diabetes. Am J Manag Care. 2010;16:413–20. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
