

Re-evaluation of low intensity pulsed ultrasound in treatment of tibial fractures (TRUST): randomized clinical trial
- PMID: 27797787
- PMCID: PMC5080447
- DOI: 10.1136/bmj.i5351
Re-evaluation of low intensity pulsed ultrasound in treatment of tibial fractures (TRUST): randomized clinical trial
Abstract
Objective: To determine whether low intensity pulsed ultrasound (LIPUS), compared with sham treatment, accelerates functional recovery and radiographic healing in patients with operatively managed tibial fractures.
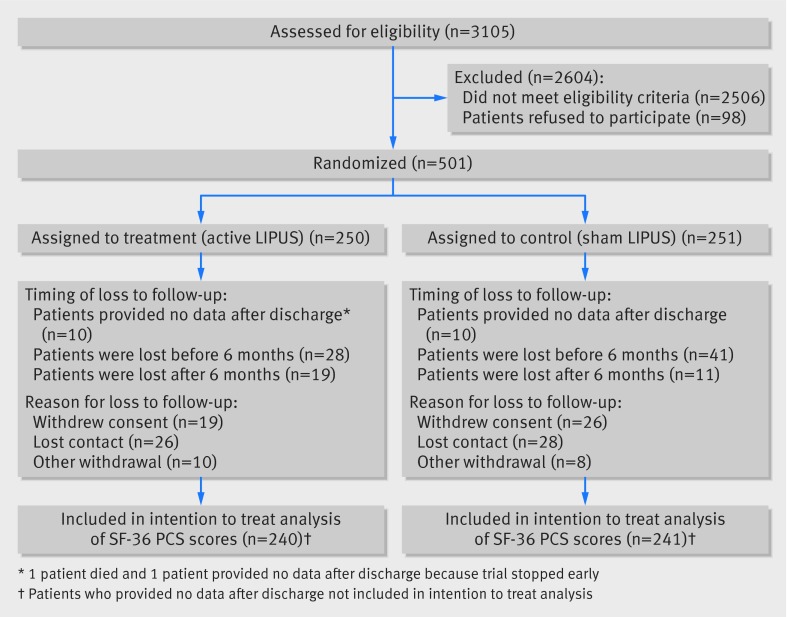
Design: A concealed, randomized, blinded, sham controlled clinical trial with a parallel group design of 501 patients, enrolled between October 2008 and September 2012, and followed for one year.
Setting: 43 North American academic trauma centers.
Participants: Skeletally mature men or women with an open or closed tibial fracture amenable to intramedullary nail fixation. Exclusions comprised pilon fractures, tibial shaft fractures that extended into the joint and required reduction, pathological fractures, bilateral tibial fractures, segmental fractures, spiral fractures >7.5 cm in length, concomitant injuries that were likely to impair function for at least as long as the patient's tibial fracture, and tibial fractures that showed <25% cortical contact and >1 cm gap after surgical fixation. 3105 consecutive patients who underwent intramedullary nailing for tibial fracture were assessed, 599 were eligible and 501 provided informed consent and were enrolled.
Interventions: Patients were allocated centrally to self administer daily LIPUS (n=250) or use a sham device (n=251) until their tibial fracture showed radiographic healing or until one year after intramedullary fixation.
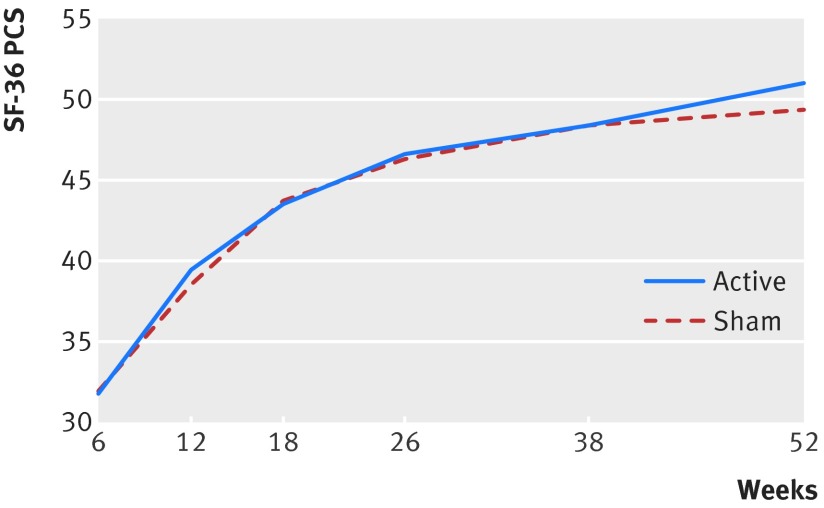
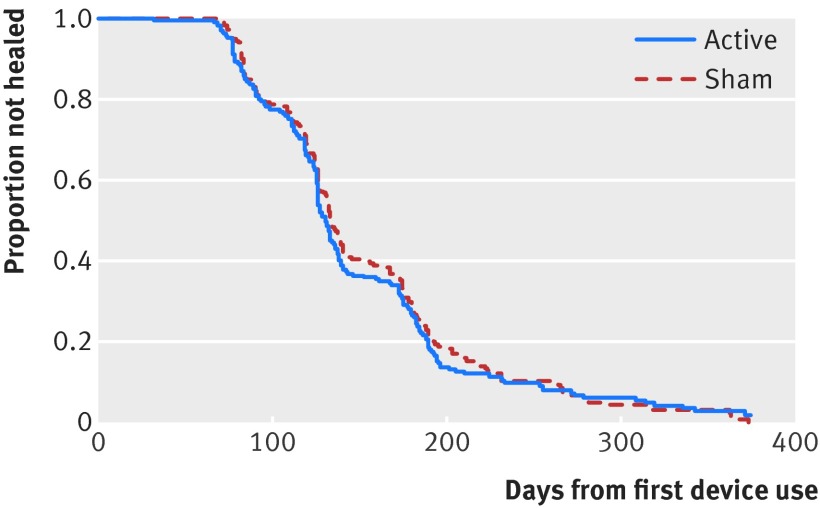
Main outcome measures: Primary registry specified outcome was time to radiographic healing within one year of fixation; secondary outcome was rate of non-union. Additional protocol specified outcomes included short form-36 (SF-36) physical component summary (PCS) scores, return to work, return to household activities, return to ≥80% of function before injury, return to leisure activities, time to full weight bearing, scores on the health utilities index (mark 3), and adverse events related to the device.
Results: SF-36 PCS data were acquired from 481/501 (96%) patients, for whom we had 2303/2886 (80%) observations, and radiographic healing data were acquired from 482/501 (96%) patients, of whom 82 were censored. Results showed no impact on SF-36 PCS scores between LIPUS and control groups (mean difference 0.55, 95% confidence interval -0.75 to 1.84; P=0.41) or for the interaction between time and treatment (P=0.30); minimal important difference is 3-5 points) or in other functional measures. There was also no difference in time to radiographic healing (hazard ratio 1.07, 95% confidence interval 0.86 to 1.34; P=0.55). There were no differences in safety outcomes between treatment groups. Patient compliance was moderate; 73% of patients administered ≥50% of all recommended treatments.
Conclusions: Postoperative use of LIPUS after tibial fracture fixation does not accelerate radiographic healing and fails to improve functional recovery.Study registration ClinicalTrialGov Identifier: NCT00667849.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: TAE, ES, and MB have received consulting fees from Smith & Nephew, the manufacturer of the study device. PT receives royalties from Smith & Nephew. GJDR is a paid consultant for Bioventus LLC, which is 51% owned by Essex Woodlands and 49% by Smith & Nephew. MB is supported, in part, by a Canada research chair, McMaster University.
Figures
Comment in
-
Low intensity pulsed ultrasound for fractures of the tibial shaft.BMJ. 2016 Oct 25;355:i5652. doi: 10.1136/bmj.i5652. BMJ. 2016. PMID: 27780808 Free PMC article.
-
In Patients with a Tibial Fracture, Low-Intensity Pulsed Ultrasound After Intramedullary Nail Fixation Did Not Accelerate Radiographic Healing or Improve Functional Recovery.J Bone Joint Surg Am. 2017 Aug 16;99(16):1394. doi: 10.2106/JBJS.17.00554. J Bone Joint Surg Am. 2017. PMID: 28816901 No abstract available.
References
-
- Heckman JD, Sarasohn-Kahn J. The economics of treating tibia fractures. The cost of delayed unions. Bull Hosp Jt Dis 1997;56:63-72.pmid:9063607. - PubMed
-
- Busse JW, Morton E, Lacchetti C, Guyatt GH, Bhandari M. Current management of tibial shaft fractures: a survey of 450 Canadian orthopedic trauma surgeons. Acta Orthop 2008;79:689-94. 10.1080/17453670810016722 pmid:18839377. - DOI - PubMed
-
- Sarmiento A, Sharpe FE, Ebramzadeh E, Normand P, Shankwiler J. Factors influencing the outcome of closed tibial fractures treated with functional bracing. Clin Orthop Relat Res 1995;(315):8-24.pmid:7634690. - PubMed
-
- Wachovia Capital Markets. Equity research: bone growth stimulation 2008 outlook. 2007.
-
- Griffin XL, Parsons N, Costa ML, Metcalfe D. Ultrasound and shockwave therapy for acute fractures in adults. Cochrane Database Syst Rev 2014;6:CD008579.pmid:24956457. - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous