

Clinicopathological features of adult-onset neuronal intranuclear inclusion disease
- PMID: 27797808
- PMCID: PMC5382941
- DOI: 10.1093/brain/aww249
Clinicopathological features of adult-onset neuronal intranuclear inclusion disease
Abstract
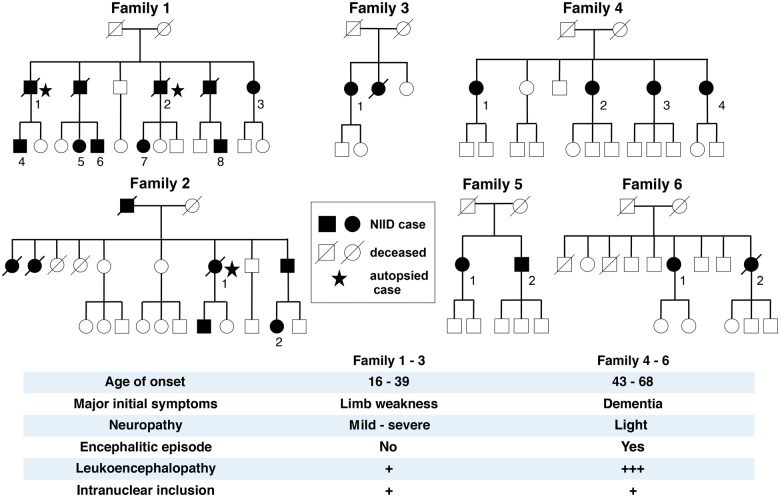
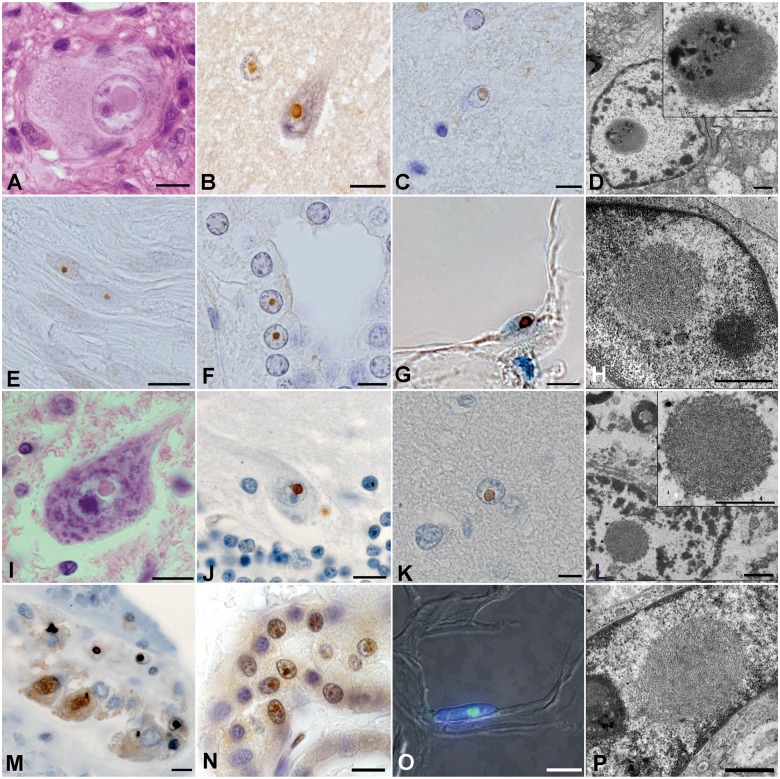
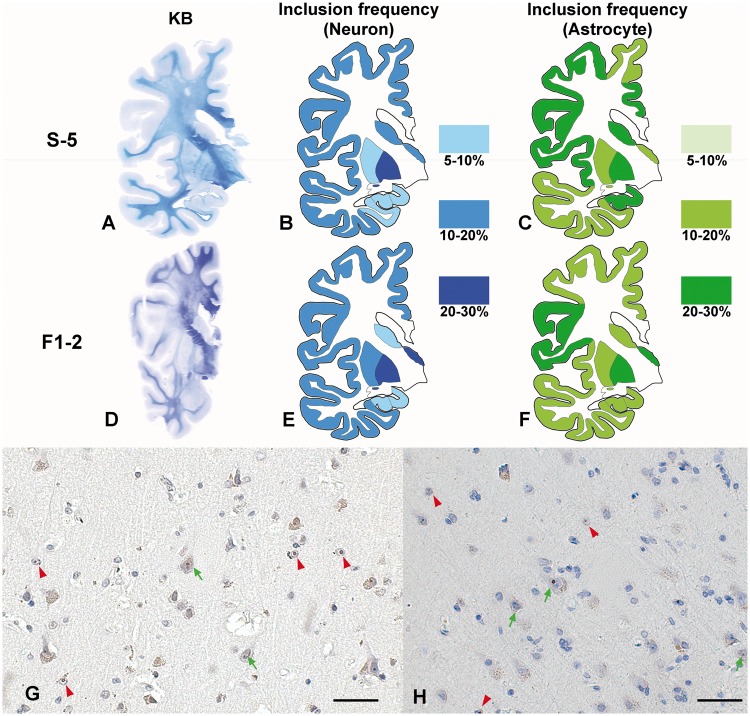
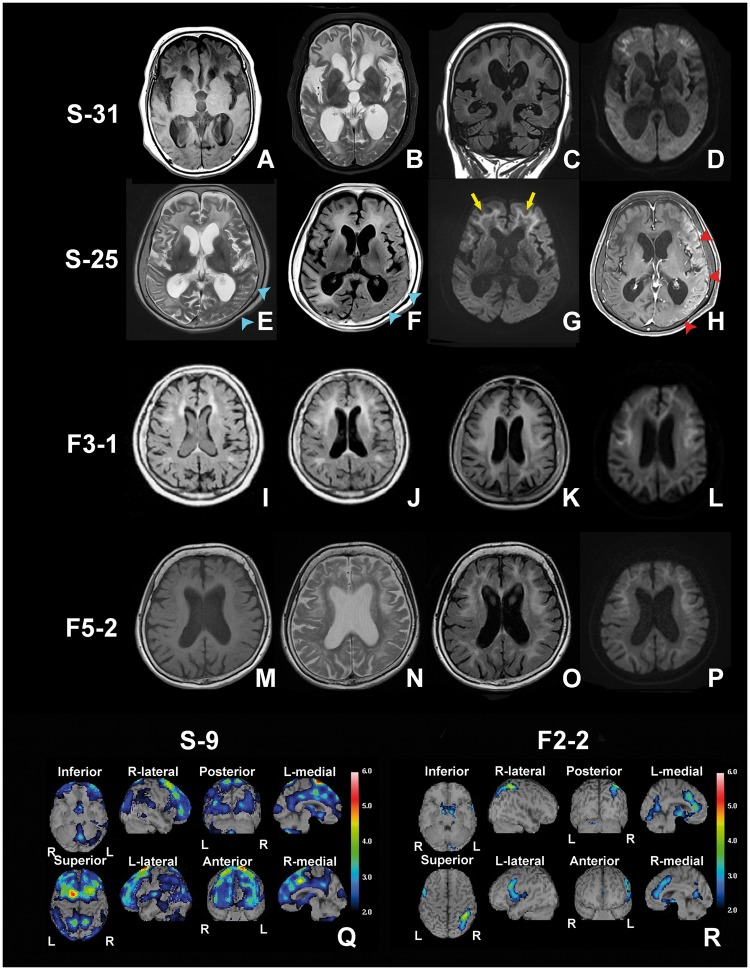
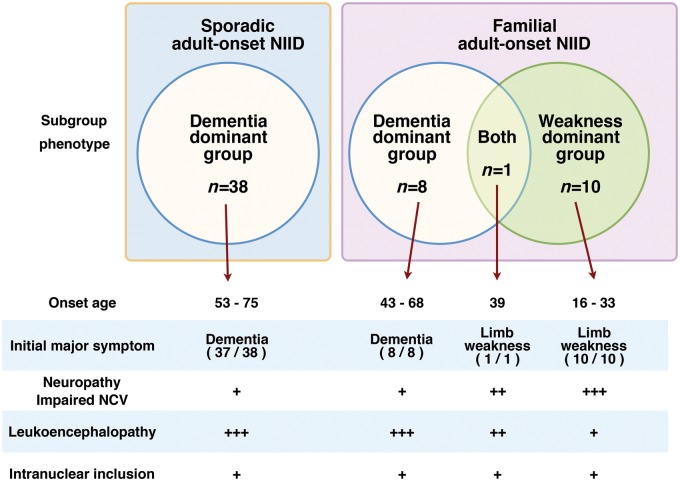
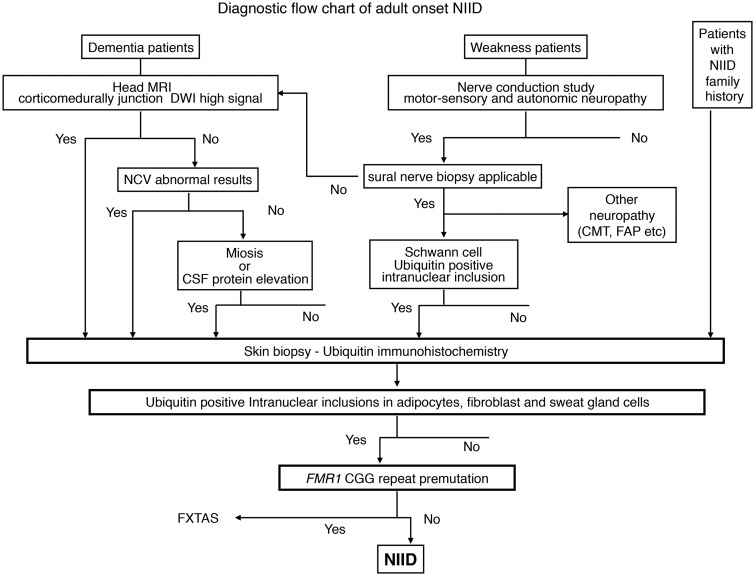
Neuronal intranuclear inclusion disease (NIID) is a slowly progressive neurodegenerative disease characterized by eosinophilic hyaline intranuclear inclusions in the central and peripheral nervous system, and also in the visceral organs. NIID has been considered to be a heterogeneous disease because of the highly variable clinical manifestations, and ante-mortem diagnosis has been difficult. However, since we reported the usefulness of skin biopsy for the diagnosis of NIID, the number of NIID diagnoses has increased, in particular adult-onset NIID. In this study, we studied 57 cases of adult-onset NIID and described their clinical and pathological features. We analysed both NIID cases diagnosed by post-mortem dissection and by ante-mortem skin biopsy based on the presence of characteristic eosinophilic, hyaline and ubiquitin-positive intanuclear inclusion: 38 sporadic cases and 19 familial cases, from six families. In the sporadic NIID cases with onset age from 51 to 76, dementia was the most prominent initial symptom (94.7%) as designated 'dementia dominant group', followed by miosis, ataxia and unconsciousness. Muscle weakness and sensory disturbance were also observed. It was observed that, in familial NIID cases with onset age less than 40 years, muscle weakness was seen most frequently (100%), as designated 'limb weakness group', followed by sensory disturbance, miosis, bladder dysfunction, and dementia. In familial cases with more than 40 years of onset age, dementia was most prominent (100%). Elevated cerebrospinal fluid protein and abnormal nerve conduction were frequently observed in both sporadic and familial NIID cases. Head magnetic resonance imaging showed high intensity signal in corticomedullary junction in diffusion-weighted image in both sporadic and familial NIID cases, a strong clue to the diagnosis. All of the dementia dominant cases presented with this type of leukoencephalopathy on head magnetic resonance imaging. Both sporadic and familial NIID cases presented with a decline in Mini-Mental State Examination and Frontal Assessment Battery scores. Based on these clinicopathological features, we proposed a diagnosis flow chart of adult-onset NIID. Our study suggested that the prevalence rate of adult-onset NIID may be higher than previously thought, and that NIID may be underdiagnosed. We should take NIID into account for differential diagnosis of leukoencephalopathy and neuropathy.
Keywords: dementia; diffusion-weighted image; intranuclear inclusion; leukoencephalopathy; skin biopsy.
© The Author (2016). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Neuronal intranuclear (hyaline) inclusion disease and fragile X-associated tremor/ataxia syndrome: a morphological and molecular dilemma.Brain. 2017 Aug 1;140(8):e51. doi: 10.1093/brain/awx156. Brain. 2017. PMID: 28899011 No abstract available.
-
Reply: Neuronal intranuclear (hyaline) inclusion disease and fragile X-associated tremor/ataxia syndrome: a morphological and molecular dilemma.Brain. 2017 Aug 1;140(8):e52. doi: 10.1093/brain/awx158. Brain. 2017. PMID: 28899012 No abstract available.
-
NOTCH2NLC-linked neuronal intranuclear inclusion body disease and fragile X-associated tremor/ataxia syndrome.Brain. 2020 Aug 1;143(8):e69. doi: 10.1093/brain/awaa210. Brain. 2020. PMID: 32789443 No abstract available.
References
-
- Appollonio I, Leone M, Isella V, Piamarta F, Consoli T, Villa ML, et al. The Frontal Assessment Battery (FAB): normative values in an Italian population sample. Neurol Sci 2005; 26: 108–16. - PubMed
-
- Barnett JL, McDonnell WM, Appelman HD, Dobbins WO. Familial visceral neuropathy with neuronal intranuclear inclusions: diagnosis by rectal biopsy. Gastroenterology 1992; 102: 684–91. - PubMed
-
- Chabriat H, Joutel A, Dichgans M, Tournier-Lasserve E, Bousser MG. Cadasil. Lancet Neurol 2009; 8: 643–53. - PubMed
-
- Dickson DW, Wertkin A, Kress Y, Ksiezak-Reding H, Yen SH. Ubiquitin immunoreactive structures in normal human brains. Distribution and developmental aspects. Lab Invest 1990; 63: 87–99. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
