

Genomic Heterogeneity and Exceptional Response to Dual Pathway Inhibition in Anaplastic Thyroid Cancer
- PMID: 27797976
- PMCID: PMC5393965
- DOI: 10.1158/1078-0432.CCR-16-2154-T
Genomic Heterogeneity and Exceptional Response to Dual Pathway Inhibition in Anaplastic Thyroid Cancer
Abstract
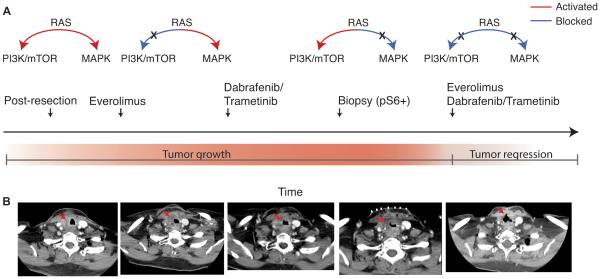
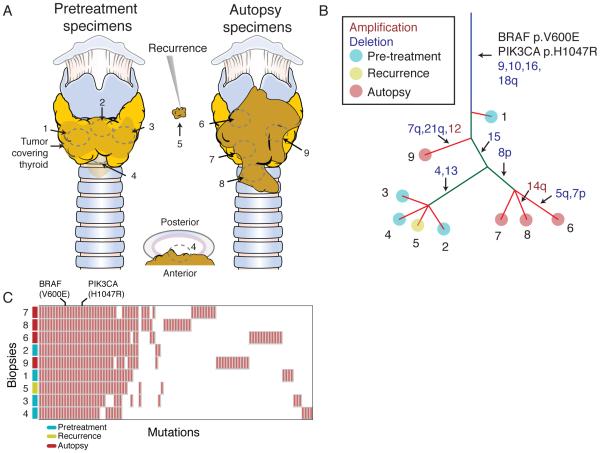
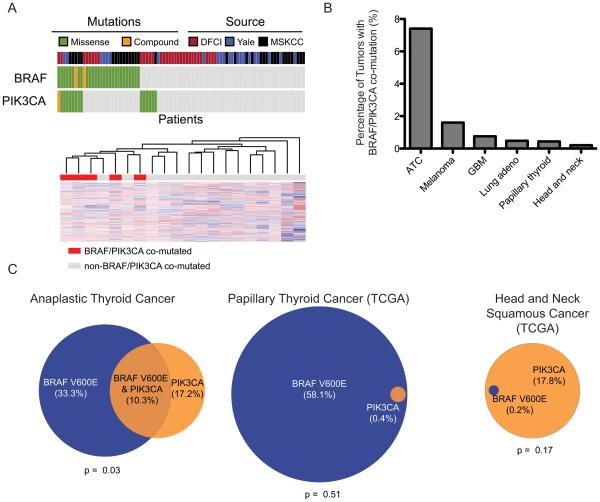
Purpose: Cancers may resist single-agent targeted therapies when the flux of cellular growth signals is shifted from one pathway to another. Blockade of multiple pathways may be necessary for effective inhibition of tumor growth. We document a case in which a patient with anaplastic thyroid carcinoma (ATC) failed to respond to either mTOR/PI3K or combined RAF/MEK inhibition but experienced a dramatic response when both drug regimens were combined.Experimental Design: Multi-region whole-exome sequencing of five diagnostic and four autopsy tumor biopsies was performed. Meta-analysis of DNA and RNA sequencing studies of ATC was performed.Results: Sequencing revealed truncal BRAF and PIK3CA mutations, which are known to activate the MAPK and PI3K/AKT pathways, respectively. Meta-analysis demonstrated 10.3% cooccurrence of MAPK and PI3K pathway alterations in ATC. These tumors display a separate transcriptional profile from other ATCs, consistent with a novel subgroup of ATC.Conclusions: BRAF and PIK3CA mutations define a distinct subset of ATC. Blockade of the MAPK and PI3K pathways appears necessary for tumor response in this subset of ATC. This identification of synergistic activity between targeted agents may inform clinical trial design in ATC. Clin Cancer Res; 23(9); 2367-73. ©2016 AACR.
©2016 American Association for Cancer Research.
Figures
References
-
- Tan RK, Finley RK, 3rd, Driscoll D, Bakamjian V, Hicks WL, Jr., Shedd DP. Anaplastic carcinoma of the thyroid: a 24-year experience. Head & neck. 1995;17:41–7. discussion 7-8. - PubMed
-
- Ito K, Hanamura T, Murayama K, Okada T, Watanabe T, Harada M, et al. Multimodality therapeutic outcomes in anaplastic thyroid carcinoma: improved survival in subgroups of patients with localized primary tumors. Head & neck. 2012;34:230–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
