

Rehabilitation Enablement in Chronic Heart Failure-a facilitated self-care rehabilitation intervention in patients with heart failure with preserved ejection fraction (REACH-HFpEF) and their caregivers: rationale and protocol for a single-centre pilot randomised controlled trial
- PMID: 27798024
- PMCID: PMC5093626
- DOI: 10.1136/bmjopen-2016-012853
Rehabilitation Enablement in Chronic Heart Failure-a facilitated self-care rehabilitation intervention in patients with heart failure with preserved ejection fraction (REACH-HFpEF) and their caregivers: rationale and protocol for a single-centre pilot randomised controlled trial
Abstract
Introduction: The Rehabilitation EnAblement in CHronic Heart Failure in patients with Heart Failure (HF) with preserved ejection fraction (REACH-HFpEF) pilot trial is part of a research programme designed to develop and evaluate a facilitated, home-based, self-help rehabilitation intervention to improve self-care and quality of life (QoL) in heart failure patients and their caregivers. We will assess the feasibility of a definitive trial of the REACH-HF intervention in patients with HFpEF and their caregivers. The impact of the REACH-HF intervention on echocardiographic outcomes and bloodborne biomarkers will also be assessed.
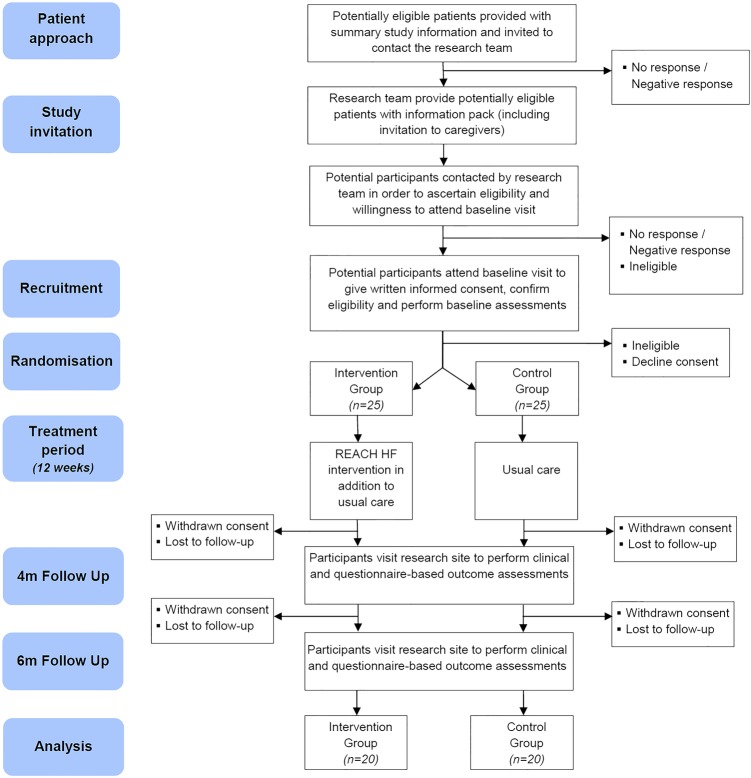
Methods and analysis: A single-centre parallel two-group randomised controlled trial (RCT) with 1:1 individual allocation to the REACH-HF intervention plus usual care (intervention) or usual care alone (control) in 50 HFpEF patients and their caregivers. The REACH-HF intervention comprises a REACH-HF manual with supplementary tools, delivered by trained facilitators over 12 weeks. A mixed methods approach will be used to assess estimation of recruitment and retention rates; fidelity of REACH-HF manual delivery; identification of barriers to participation and adherence to the intervention and study protocol; feasibility of data collection and outcome burden. We will assess the variance in study outcomes to inform a definitive study sample size and assess methods for the collection of resource use and intervention delivery cost data to develop the cost-effectiveness analyses framework for any future trial. Patient outcomes collected at baseline, 4 and 6 months include QoL, psychological well-being, exercise capacity, physical activity and HF-related hospitalisation. Caregiver outcomes will also be assessed, and a substudy will evaluate impact of the REACH-HF manual on resting global cardiovascular function and bloodborne biomarkers in HFpEF patients.
Ethics and dissemination: The study is approved by the East of Scotland Research Ethics Service (Ref: 15/ES/0036). Findings will be disseminated via journals and presentations to clinicians, commissioners and service users.
Trial registration number: ISRCTN78539530; Pre-results .
Keywords: Cardiac Rehabilitation; Caregivers; Complex Intervention; Preserved Ejection Fraction; Randomised Controlled Trial.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare: RST is the lead for the ongoing portfolio of Cochrane reviews of cardiac rehabilitation. RST and HMD are named topic specific experts for the NICE clinical guidelines update in heart failure. HD is an ordinary member of the British Association for Cardiovascular Prevention and Rehabilitation (BACPR) council.
References
-
- Kitzman DW, Little WC, Brubaker PH et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA 2002;288:2144–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous