

Contemporary Patterns of Multiple Organ Dysfunction in Trauma
- PMID: 27798537
- PMCID: PMC5398901
- DOI: 10.1097/SHK.0000000000000779
Contemporary Patterns of Multiple Organ Dysfunction in Trauma
Erratum in
-
Contemporary Patterns of Multiple Organ Dysfunction in Trauma: Erratum.Shock. 2017 Jul;48(1):139. doi: 10.1097/SHK.0000000000000881. Shock. 2017. PMID: 28608785 Free PMC article. No abstract available.
Abstract
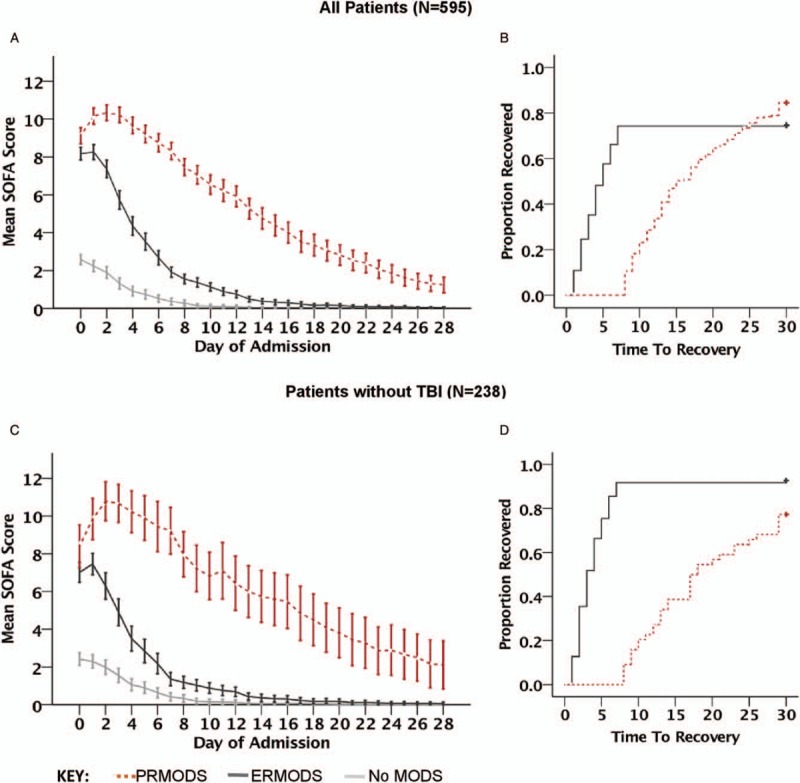
Background: Multiple organ dysfunction syndrome (MODS) is associated with poor outcomes for trauma patients. Different forms of MODS may exist and have different consequences. The ability to distinguish them clinically may have implications for prognosis and treatment. We wished to study whether prolonged MODS (PRMODS) could be observed as a distinct clinical entity to early resolving MODS (ERMODS) in critically injured patients.
Methods: Adult major trauma patients recruited to a prospective observational study at a single major trauma center were eligible for inclusion. MODS was defined as Sequential Organ Failure Assessment (SOFA) score >5; and PRMODS as lasting >7 days. Time to recovery (TTR) was calculated as the number of days before the SOFA fell below the MODS threshold (≤5).
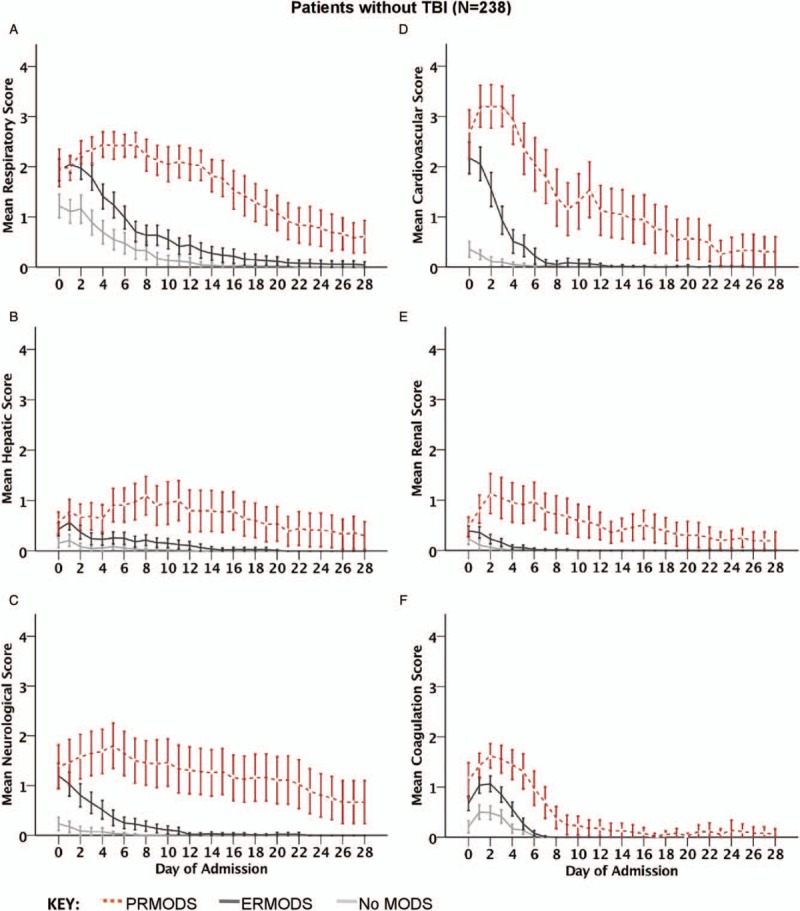
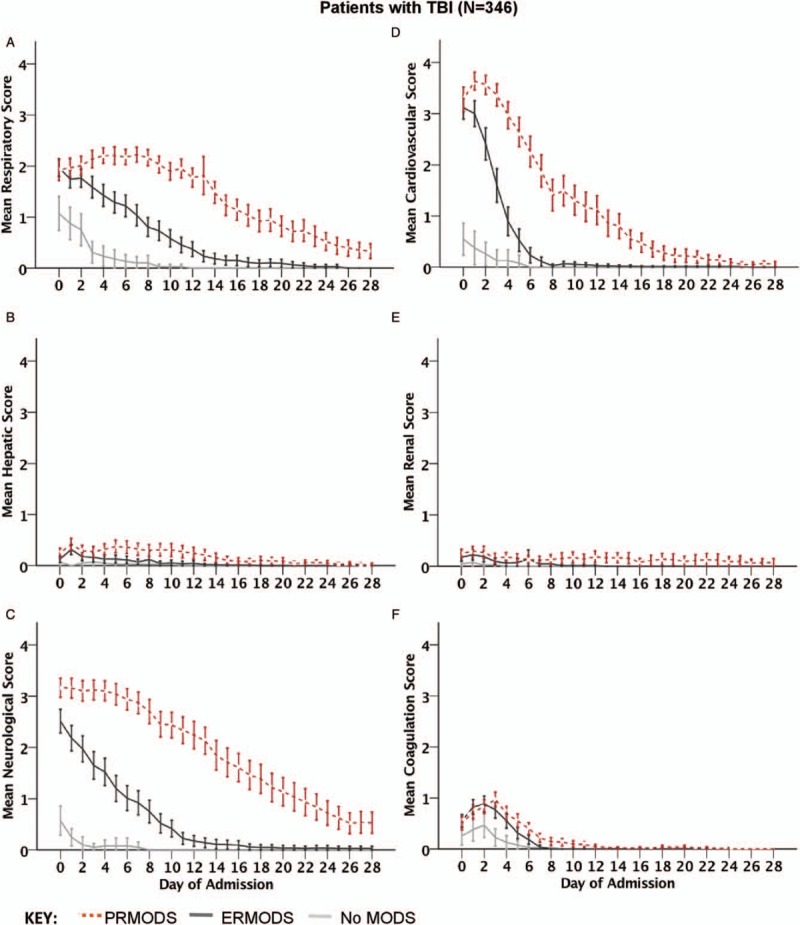
Results: Five hundred ninety-five patients were enrolled of whom 285 developed ERMODS (48%) and 184 (31%) PRMODS. Organ dysfunction was more severe and protracted in PRMODS, especially in patients without brain injury (mean SOFA 11 vs. 6, Day 2, P < 0.001; TTR 17 vs. 3 days, P < 0.001). PRMODS exhibited higher rates of hepatic and renal dysfunction (84% vs. 56%; and 78% vs. 47%, P≤0.001). Patterns of recovery were distinct in hepatic, renal, and neurological systems (TTR 15 vs. 4; 20 vs. 3; and 28 vs. 7 days, P < 0.01). PRMODS was associated with higher infection and mortality rates (91% vs. 41%; and 22% vs. 7%, P < 0.001).
Conclusion: PRMODS appears common, a distinct clinical entity, and associated with worse patient outcomes. PRMODS may represent an important endpoint for studies evaluating outcomes following trauma.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Fröhlich M, Lefering R, Probst C, Paffrath T, Schneider MM, Maegele M, Sakka SG, Bouillon B, Wafaisade A. Committee on Emergency Medicine, Intensive Care and Trauma Management of the German Trauma Society Sektion NIS.. Epidemiology and risk factors of multiple-organ failure after multiple trauma: An analysis of 31,154 patients from the TraumaRegister DGU. J Trauma Acute Care Surg 2014; 76:921–928. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
