

A Latent Class Analysis to Identify Variation in Caregivers' Preferences for their Child's Attention-Deficit/Hyperactivity Disorder Treatment: Do Stated Preferences Match Current Treatment?
- PMID: 27798814
- PMCID: PMC6029258
- DOI: 10.1007/s40271-016-0202-z
A Latent Class Analysis to Identify Variation in Caregivers' Preferences for their Child's Attention-Deficit/Hyperactivity Disorder Treatment: Do Stated Preferences Match Current Treatment?
Abstract
Objectives: To investigate variation in caregiver preferences for their child's attention-deficit/hyperactivity disorder (ADHD) care and to determine if their stated preferences align with current care management.
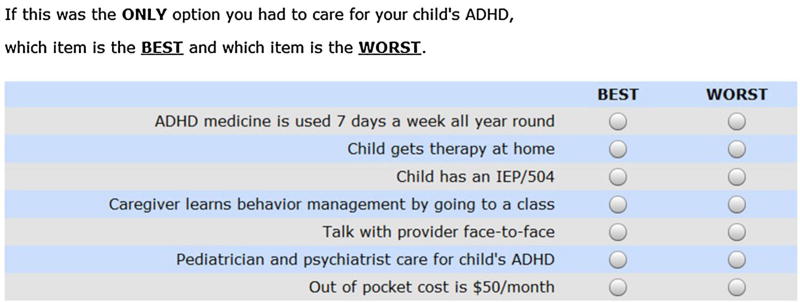
Methods: Caregivers of a child aged 4-14 years and in care for ADHD were recruited from pediatric outpatient clinics and advocacy groups across the state of Maryland. Participants completed a survey collecting demographics, the child's treatment, and caregiver preferences-elicited using a best-worst scaling experiment (case 2). Latent class analysis was used to identify distinct preference segments and bivariate analyses were used to compare the association between segment membership with what the child was currently receiving for their ADHD.
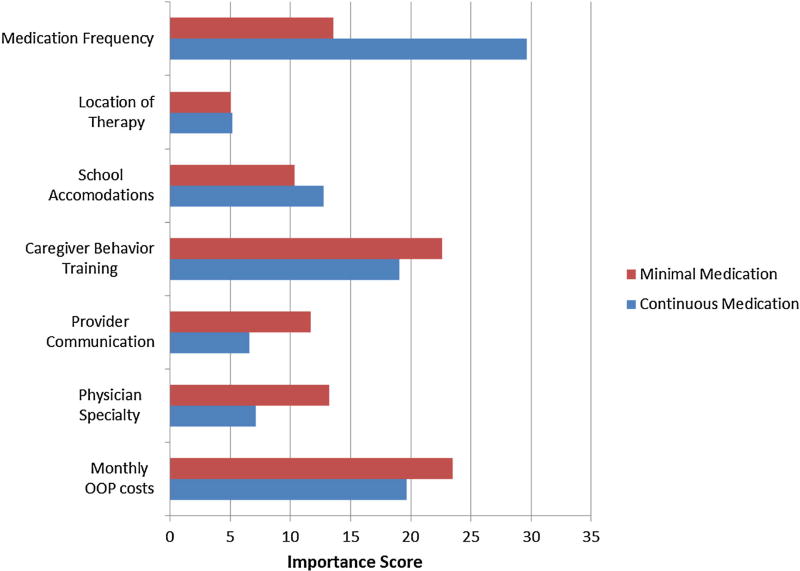
Results: Participants (n = 184) were predominantly White (68%) and the child's mother (84%). Most children had ADHD for 2 or more years (79%). Caregiver preferences were distinguished by two segments: continuous medication (36%) and minimal medication (64%). The two groups had very different preferences for when medication was administered (p < 0.001), but they had similar preferences for provider-oriented and non-medication interventions (p > 0.05 for the caregiver behavior training, provider communication, provider specialty, and out-of-pocket costs). One third of the sample did not receive the preferred individualized education program and 42% of the minimal medication group reported using medication 7 days a week all year round.
Conclusions: Although behavior management training and school accommodations aspects of an ADHD care plan are more important to caregivers than evidence-based medication, fewer families had access to educational accommodations. Further research is needed to clarify how stated preferences for care align with treatments used in actual practice settings.
Conflict of interest statement
Figures
Similar articles
-
Caregiver Treatment Preferences for Children with a New Versus Existing Attention-Deficit/Hyperactivity Disorder Diagnosis.J Child Adolesc Psychopharmacol. 2017 Apr;27(3):234-242. doi: 10.1089/cap.2016.0157. Epub 2016 Dec 19. J Child Adolesc Psychopharmacol. 2017. PMID: 27991834 Free PMC article.
-
Using Best-Worst Scaling to Measure Caregiver Preferences for Managing their Child's ADHD: A Pilot Study.Patient. 2015 Oct;8(5):423-31. doi: 10.1007/s40271-014-0098-4. Patient. 2015. PMID: 25392024 Free PMC article.
-
Caregivers' Priorities and Observed Outcomes of Attention-Deficit Hyperactivity Disorder Medication for Their Children.J Dev Behav Pediatr. 2018 Feb/Mar;39(2):93-100. doi: 10.1097/DBP.0000000000000530. J Dev Behav Pediatr. 2018. PMID: 29461996 Free PMC article.
-
Assessment of parents' preferences for the treatment of school-age children with ADHD: a discrete choice experiment.Expert Rev Pharmacoecon Outcomes Res. 2011 Jun;11(3):245-52. doi: 10.1586/erp.11.22. Expert Rev Pharmacoecon Outcomes Res. 2011. PMID: 21671692 Review.
-
Treatment of attention-deficit/hyperactivity disorder: overview of the evidence.Pediatrics. 2005 Jun;115(6):e749-57. doi: 10.1542/peds.2004-2560. Pediatrics. 2005. PMID: 15930203 Review.
Cited by
-
Parents matter: Parent acceptance of school-based executive functions interventions relates to improved child outcomes.J Clin Psychol. 2022 Jul;78(7):1388-1406. doi: 10.1002/jclp.23309. Epub 2022 Jan 8. J Clin Psychol. 2022. PMID: 34997971 Free PMC article.
-
A comparative study on the neurophysiological mechanisms underlying effects of methylphenidate and neurofeedback on inhibitory control in attention deficit hyperactivity disorder.Neuroimage Clin. 2018;20:1191-1203. doi: 10.1016/j.nicl.2018.10.027. Epub 2018 Oct 25. Neuroimage Clin. 2018. PMID: 30390574 Free PMC article.
-
Stakeholder-Engaged Derivation of Patient-Informed Value Elements.Patient. 2020 Oct;13(5):611-621. doi: 10.1007/s40271-020-00433-8. Patient. 2020. PMID: 32676998 Free PMC article.
-
Using Latent Class Analysis to Model Preference Heterogeneity in Health: A Systematic Review.Pharmacoeconomics. 2018 Feb;36(2):175-187. doi: 10.1007/s40273-017-0575-4. Pharmacoeconomics. 2018. PMID: 28975582
-
Adult Patient Preferences for Long-Acting ADHD Treatments: A Discrete Choice Experiment.Patient Prefer Adherence. 2021 May 21;15:1061-1073. doi: 10.2147/PPA.S311836. eCollection 2021. Patient Prefer Adherence. 2021. PMID: 34054292 Free PMC article.
References
-
- The MTA Cooperative Group. National Institute of Mental Health Multimodal Treatment Study of ADHD follow-up: 24-month outcomes of treatment strategies for attention-deficit/hyperactivity disorder. Pediatrics. 2004;113(4):754–61. - PubMed
-
- Wolraich ML, Greenhill LL, Pelham W, et al. Randomized, controlled trial of oros methylphenidate once a day in children with attention-deficit/hyperactivity disorder. Pediatrics. 2001;108(4):883–92. - PubMed
-
- The MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder: the MTA Cooperative Group. Multimodal Treatment Study of Children with ADHD. Arch Gen Psychiatry. 1999;56(12):1073–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
