

Associations between adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and biomarkers of inflammation, hormonal, and insulin response
- PMID: 27798951
- PMCID: PMC5167632
- DOI: 10.1002/ijc.30494
Associations between adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and biomarkers of inflammation, hormonal, and insulin response
Abstract
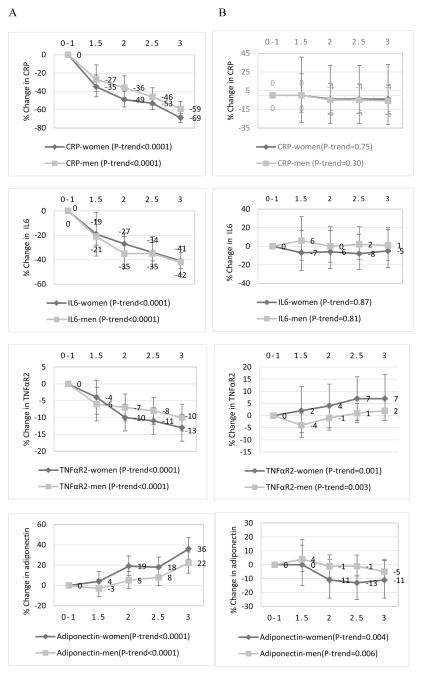
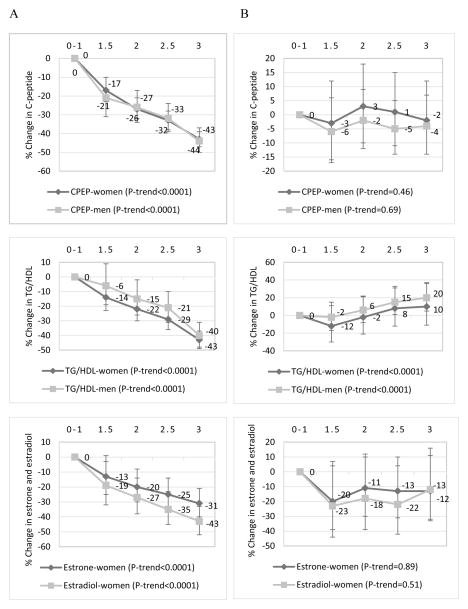
Adherence to the 2007 WCRF/AICR cancer prevention recommendations has been associated with lower cancer risk but the underlying biological mechanisms have not been elucidated. We utilized dietary and lifestyle data from 11,342 women in the Nurses' Health Study and 8,136 men in the Health Professionals Follow-up Study, to investigate associations between adherence scores and markers of inflammation, hormonal and insulin response. Two scores ranging from 0 to 3 were constructed to assess adherence to the energy balance-related recommendations (weight management, physical activity, energy density); and the plant, animal foods and alcohol intake recommendations; with higher scores indicating greater adherence. The following biomarkers were assessed in plasma samples donated by chronic disease-free women (1990) and men (1994): C-reactive protein (CRP), interleukin (IL)-6, tumor necrosis factor (TNF)-α receptor 2 (TNFαR2) and adiponectin for inflammation; estrone and estradiol for hormonal response in women, C-peptide for hyperinsulinemia; and triglycerides/high density lipoprotein-cholesterol (TG/HDL) ratio for insulin resistance. In multivariable-adjusted linear regression analyses, we estimated relative concentrations of biomarkers across adherence categories. There was a significant trend of lower (higher for adiponectin) biomarker concentrations with higher adherence to the energy balance recommendations (all p trend <0.0001). Comparing the highest (3) to the lowest recommendation category (0-1), the percent difference in relative concentrations of biomarkers was CRP, -69%; IL6, -41%; TNFαR2, -13%; adiponectin, +36%; C-peptide, -43%; TG/HDL, -43%; estrone, -31%; and estradiol, -43%; in women; and CRP, -59%; IL6, -42%; TNFαR2, -10%; adiponectin, +22%; C-peptide, -44%; and TG/HDL, -40%; in men. In contrast, associations between adherence to the plant, animal foods and alcohol intake recommendations and biomarker concentrations were weaker, and mostly nonsignificant. The healthier biomarker profile associated with greater adherence to the WCRF/AICR cancer prevention recommendations is driven mainly by adherence to the energy balance-related recommendations.
Keywords: WCRF/AICR recommendations; cancer prevention; chronic inflammation; diet; hormones; hyperinsulinemia; insulin resistance; lifestyle.
© 2016 UICC.
Conflict of interest statement
All authors declare no conflict of interest.
Figures
References
-
- World Cancer Research Fund / American Institute for Cancer Research. WCRF/AICR Expert Report: Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective. American Institute for Cancer Research; 2007.
-
- Fanidi A, Ferrari P, Biessy C, Ortega C, Angeles-Llerenas A, Torres-Mejia G, Romieu I. Adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and breast cancer risk in the Cancer de Màma (CAMA) study. Public Health Nutrition. 2015;18:3337–48. - PMC - PubMed
-
- Romaguera D, Vergnaud AC, Peeters PH, van Gils CHCD, Ferrari P, Romieu I, Jenab M, Slimani N, Clavel-Chapelon F, Fagherazzi G, Perquier F, Kaaks R, Teucher B, Boeing H, von Rüsten A, Tjønneland A, Olsen A, Dahm CC, Overvad K, Quirós JR, Gonzalez CA, Sánchez MJ, Navarro C, Barricarte A, Dorronsoro M, Khaw KT, Wareham NJ, Crowe FL, Key TJ, Trichopoulou A, Lagiou P, Bamia C, Masala G, Vineis P, Tumino R, Sieri S, Panico S, May AM, Bueno-de-Mesquita HB, Büchner FL, Wirfält E, Manjer J, Johansson I, Hallmans G, Skeie G, Benjaminsen Borch K, Parr CL, Riboli E, Norat T. Is Concordance with World Cancer Research Fund/American Institute for Cancer Research Guidelines for Cancer Prevention Related to Subsequent Risk of Cancer? Results from the EPIC Study. The American Journal of Clinical Nutrition. 2012;96:150–63. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
