

Anatomical configurations associated with posthemorrhagic hydrocephalus among premature infants with intraventricular hemorrhage
- PMID: 27798978
- PMCID: PMC5510987
- DOI: 10.3171/2016.8.FOCUS16241
Anatomical configurations associated with posthemorrhagic hydrocephalus among premature infants with intraventricular hemorrhage
Abstract
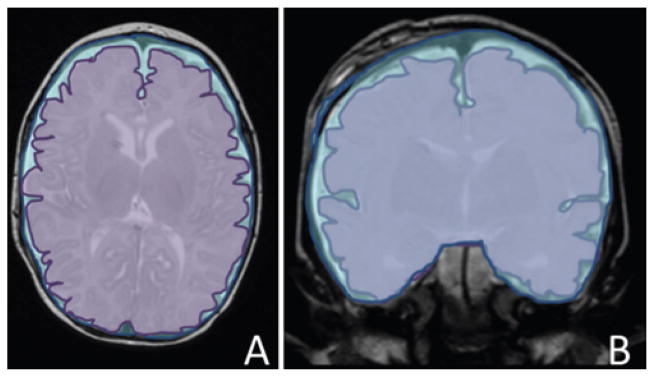
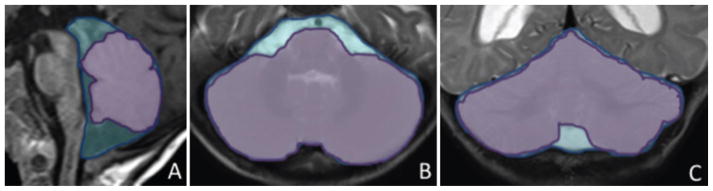
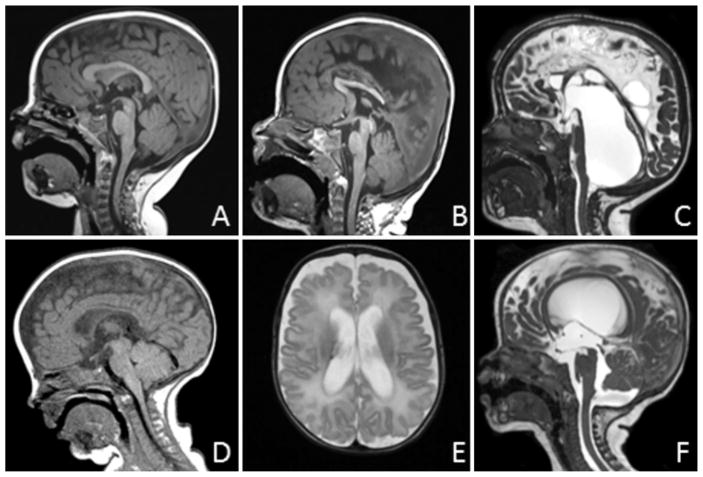
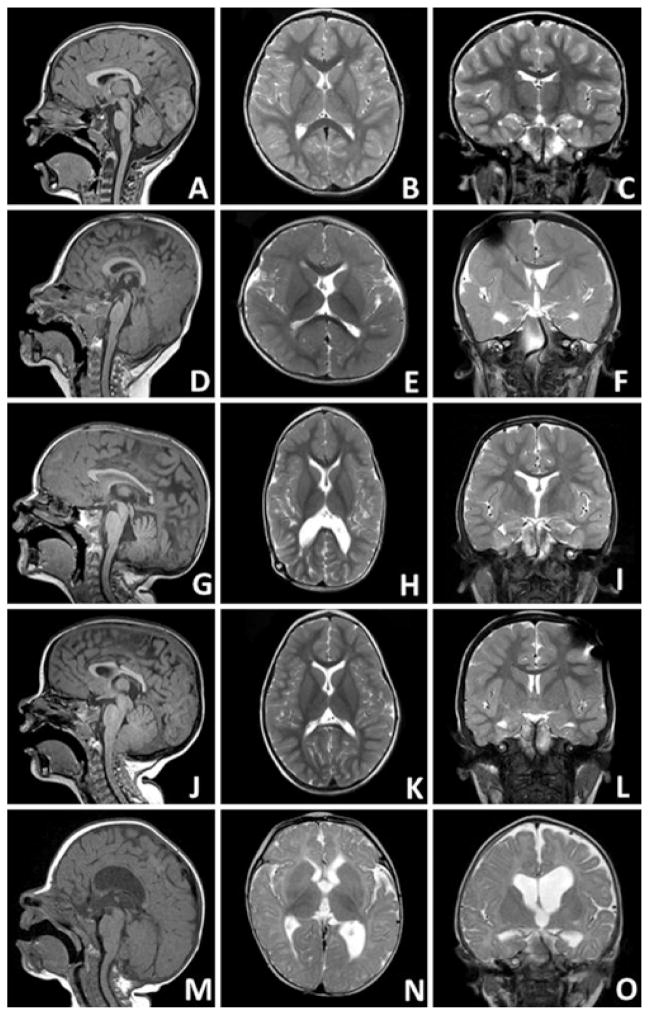
OBJECTIVE Intraventricular hemorrhage (IVH) is a complication of prematurity often associated with ventricular dilation, which may resolve over time or progress to posthemorrhagic hydrocephalus (PHH). This study investigated anatomical factors that could predispose infants with IVH to PHH. METHODS The authors analyzed a cohort of premature infants diagnosed with Grade III or IV IVH between 2004 and 2014. Using existing ultrasound and MR images, the CSF obstruction pattern, skull shape, and brain/skull ratios were determined, comparing children with PHH to those with resolved ventricular dilation (RVD), and comparing both groups to a set of healthy controls. RESULTS Among 110 premature infants with Grade III or IV IVH, 65 (59%) developed PHH. Infants with PHH had more severe ventricular dilation compared with those with RVD, although ranges overlapped. Intraventricular CSF obstruction was observed in 36 (86%) of 42 infants with PHH and 0 (0%) of 18 with RVD (p < 0.001). The distribution of skull shapes in infants with PHH was similar to those with RVD, although markedly different from controls. No significant differences in supratentorial brain/skull ratio were observed; however, the mean infratentorial brain/skull ratio of infants with PHH was 5% greater (more crowded) than controls (p = 0.006), whereas the mean infratentorial brain/skull ratio of infants with RVD was 8% smaller (less crowded) than controls (p = 0.004). CONCLUSIONS Among premature infants with IVH, intraventricular obstruction and infratentorial crowding are strongly associated with PHH, further underscoring the need for brain MRI in surgical planning. Prospective studies are required to determine which factors are cause and which are consequence, and which can be used to predict the need for surgical intervention.
Keywords: CPC = choroid plexus cauterization; ETV = endoscopic third ventriculostomy; IVH = intraventricular hemorrhage; PHH = posthemorrhagic hydrocephalus; RVD = resolved ventricular dilation; intraventricular hemorrhage; posthemorrhagic hydrocephalus; prematurity.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
Similar articles
-
Shunting outcomes in posthemorrhagic hydrocephalus: results of a Hydrocephalus Clinical Research Network prospective cohort study.J Neurosurg Pediatr. 2017 Jul;20(1):19-29. doi: 10.3171/2017.1.PEDS16496. Epub 2017 Apr 28. J Neurosurg Pediatr. 2017. PMID: 28452657
-
Temporal trends of intraventricular hemorrhage of prematurity in Nova Scotia from 1993 to 2012.J Neurosurg Pediatr. 2015 Jun;15(6):573-9. doi: 10.3171/2014.11.PEDS14363. Epub 2015 Mar 13. J Neurosurg Pediatr. 2015. PMID: 26030328
-
Impact of intraventricular hemorrhage symmetry on endoscopic third ventriculostomy with choroid plexus cauterization for posthemorrhagic hydrocephalus: an institutional experience of 50 cases.J Neurosurg Pediatr. 2022 Dec 30;31(3):245-251. doi: 10.3171/2022.12.PEDS22492. Print 2023 Mar 1. J Neurosurg Pediatr. 2022. PMID: 36585872
-
Early intervention and neurodevelopmental outcome of infants with posthemorrhagic hydrocephalus: A case series and literature review.Clin Neurol Neurosurg. 2021 Feb;201:106432. doi: 10.1016/j.clineuro.2020.106432. Epub 2020 Dec 17. Clin Neurol Neurosurg. 2021. PMID: 33383466 Review.
-
Neonatal posthemorrhagic hydrocephalus from prematurity: pathophysiology and current treatment concepts.J Neurosurg Pediatr. 2012 Mar;9(3):242-58. doi: 10.3171/2011.12.PEDS11136. J Neurosurg Pediatr. 2012. PMID: 22380952 Free PMC article. Review.
Cited by
-
Pathophysiologic mechanisms and strategies for the treatment of post-hemorrhagic hydrocephalus of prematurity.Childs Nerv Syst. 2022 Mar;38(3):511-520. doi: 10.1007/s00381-021-05427-x. Epub 2022 Jan 4. Childs Nerv Syst. 2022. PMID: 34981170
-
Intraventricular haemorrhage and posthaemorrhagic ventricular dilatation: moving beyond CSF diversion.Childs Nerv Syst. 2021 Nov;37(11):3375-3383. doi: 10.1007/s00381-021-05206-8. Epub 2021 May 15. Childs Nerv Syst. 2021. PMID: 33993367 Free PMC article. Review.
-
Bloody Ventriculography: Intracerebral Hemorrhage Artistically Casting the Ventricular System's Anatomy Into a Bird's Head.Cureus. 2022 Mar 14;14(3):e23165. doi: 10.7759/cureus.23165. eCollection 2022 Mar. Cureus. 2022. PMID: 35444877 Free PMC article.
-
Paediatric hydrocephalus.Nat Rev Dis Primers. 2024 May 16;10(1):35. doi: 10.1038/s41572-024-00519-9. Nat Rev Dis Primers. 2024. PMID: 38755194 Free PMC article. Review.
-
Inflammatory hydrocephalus.Childs Nerv Syst. 2021 Nov;37(11):3341-3353. doi: 10.1007/s00381-021-05255-z. Epub 2021 Jun 23. Childs Nerv Syst. 2021. PMID: 34164718
References
-
- Bergsneider M. Evolving concepts of cerebrospinal fluid physiology. Neurosurg Clin N Am. 2001;12:631–638. vii. - PubMed
-
- Brouwer AJ, Brouwer MJ, Groenendaal F, Benders MJ, Whitelaw A, de Vries LS. European perspective on the diagnosis and treatment of posthaemorrhagic ventricular dilatation. Arch Dis Child Fetal Neonatal Ed. 2012;97:F50–F55. - PubMed
-
- Brouwer MJ, de Vries LS, Pistorius L, Rademaker KJ, Groenendaal F, Benders MJ. Ultrasound measurements of the lateral ventricles in neonates: why, how and when? A systematic review. Acta Paediatr. 2010;99:1298–1306. - PubMed
-
- Kulkarni AV, Drake JM, Kestle JR, Mallucci CL, Sgouros S, Constantini S. Predicting who will benefit from endoscopic third ventriculostomy compared with shunt insertion in childhood hydrocephalus using the ETV Success Score. J Neurosurg Pediatr. 2010;6:310–315. - PubMed
-
- Mazzola CA, Choudhri AF, Auguste KI, Limbrick DD, Jr, Rogido M, Mitchell L, et al. Pediatric hydrocephalus: systematic literature review and evidence-based guidelines. Part 2: Management of posthemorrhagic hydrocephalus in premature infants. J Neurosurg Pediatr. 2014;14(Suppl 1):8–23. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
