

Hypertension-Linked Pathophysiological Alterations in the Gut
- PMID: 27799253
- PMCID: PMC5250568
- DOI: 10.1161/CIRCRESAHA.116.309006
Hypertension-Linked Pathophysiological Alterations in the Gut
Abstract
Rationale: Sympathetic nervous system control of inflammation plays a central role in hypertension. The gut receives significant sympathetic innervation, is densely populated with a diverse microbial ecosystem, and contains immune cells that greatly impact overall inflammatory homeostasis. Despite this uniqueness, little is known about the involvement of the gut in hypertension.
Objective: Test the hypothesis that increased sympathetic drive to the gut is associated with increased gut wall permeability, increased inflammatory status, and microbial dysbiosis and that these gut pathological changes are linked to hypertension.
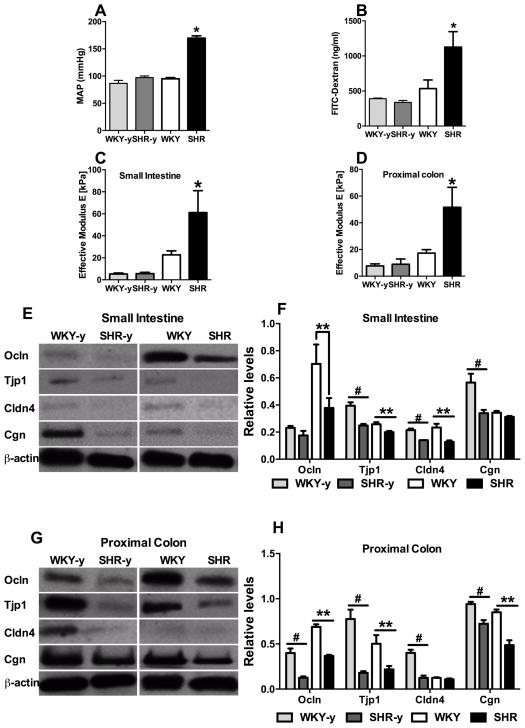
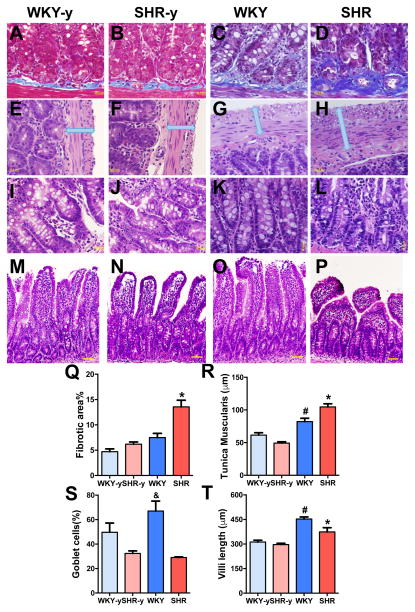
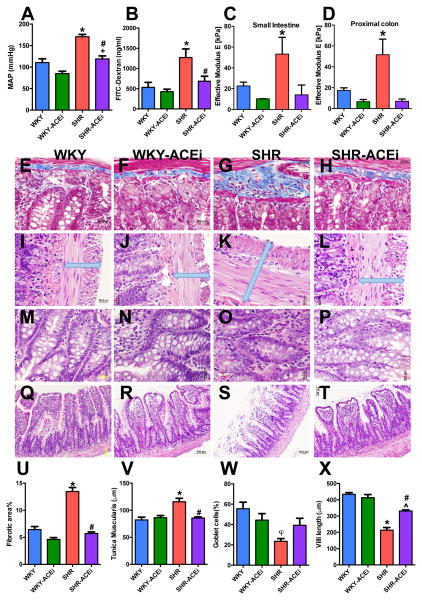
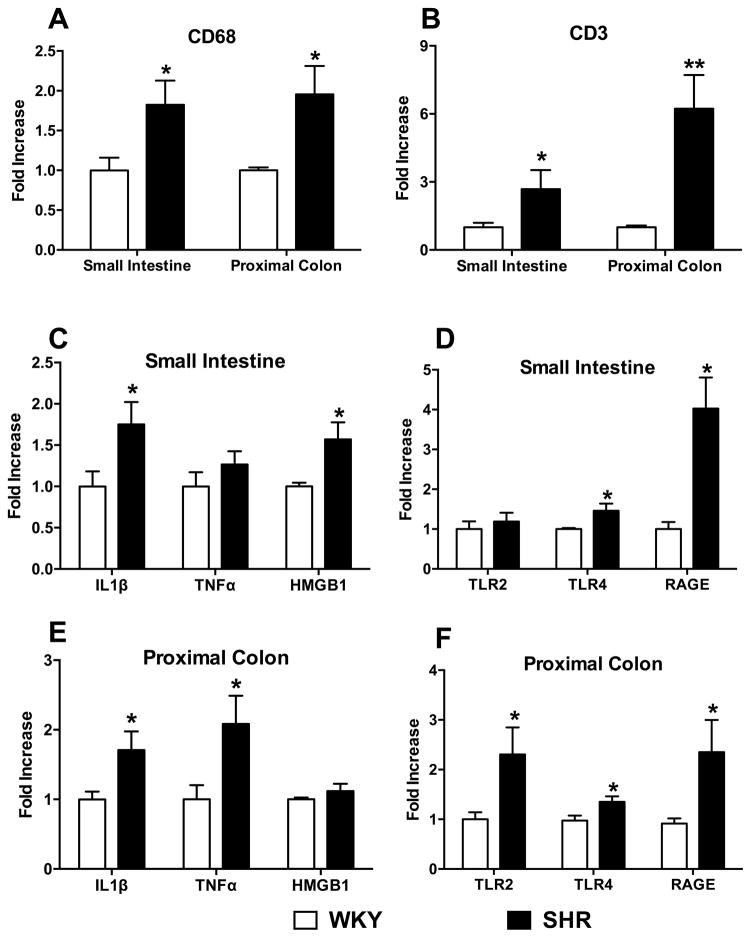
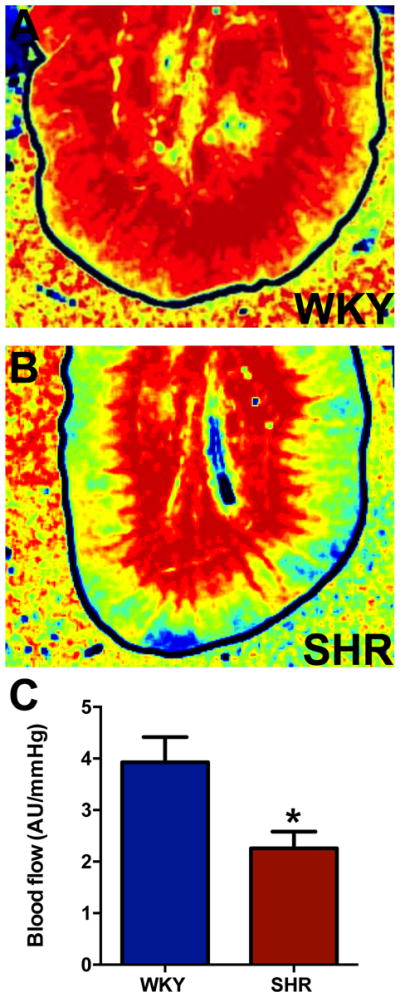
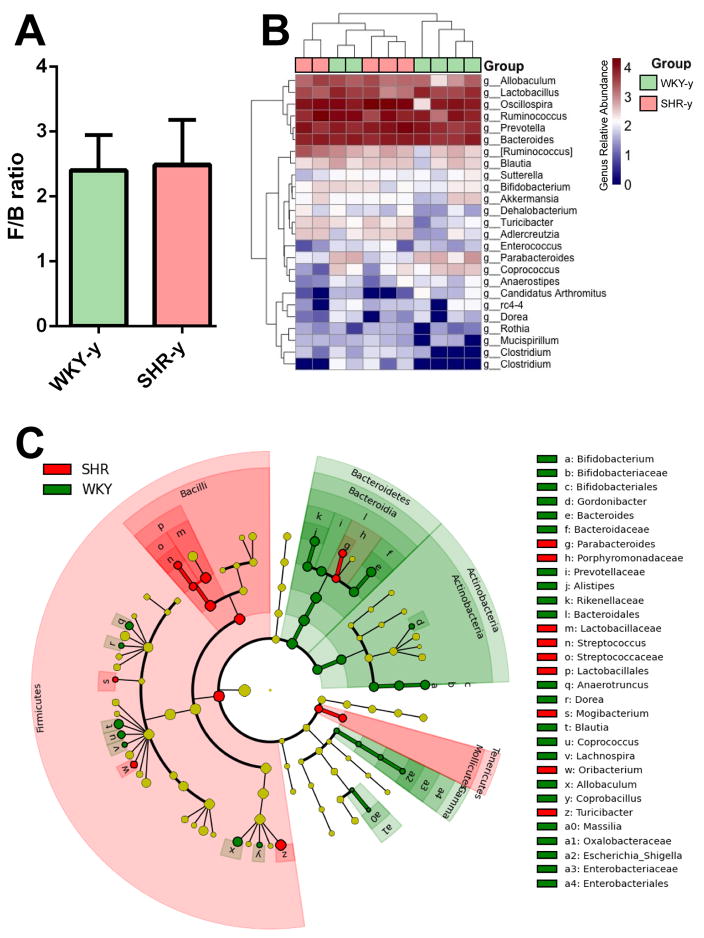
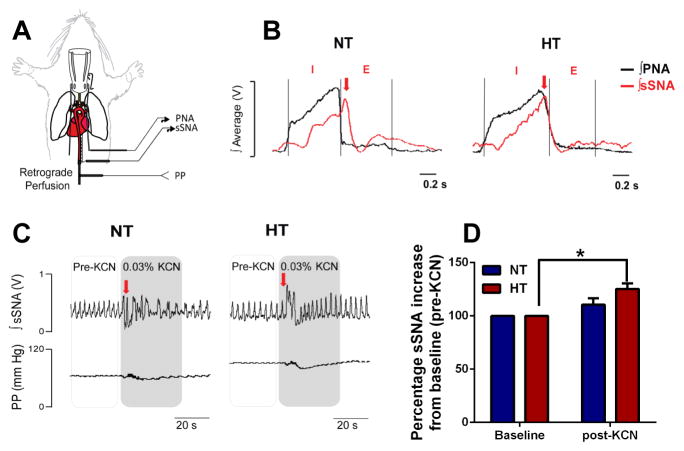
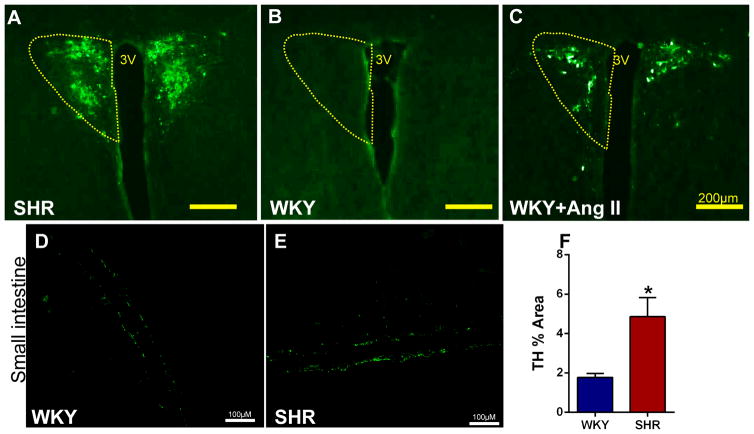
Methods and results: Gut epithelial integrity and wall pathology were examined in spontaneously hypertensive rat and chronic angiotensin II infusion rat models. The increase in blood pressure in spontaneously hypertensive rat was associated with gut pathology that included increased intestinal permeability and decreased tight junction proteins. These changes in gut pathology in hypertension were associated with alterations in microbial communities relevant in blood pressure control. We also observed enhanced gut-neuronal communication in hypertension originating from paraventricular nucleus of the hypothalamus and presenting as increased sympathetic drive to the gut. Finally, angiotensin-converting enzyme inhibition (captopril) normalized blood pressure and was associated with reversal of gut pathology.
Conclusions: A dysfunctional sympathetic-gut communication is associated with gut pathology, dysbiosis, and inflammation and plays a key role in hypertension. Thus, targeting of gut microbiota by innovative probiotics, antibiotics, and fecal transplant, in combination with the current pharmacotherapy, may be a novel strategy for hypertension treatment.
Keywords: autonomic nervous system; gut; hypertension; inflammation; intestines; microbiota.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
Hypertension: Microbiota under pressure.Nat Rev Nephrol. 2017 Jan;13(1):3. doi: 10.1038/nrneph.2016.173. Epub 2016 Nov 21. Nat Rev Nephrol. 2017. PMID: 27867190 No abstract available.
-
Hypertension Opens the Flood Gates to the Gut Microbiota.Circ Res. 2017 Jan 20;120(2):249-251. doi: 10.1161/CIRCRESAHA.116.310339. Circ Res. 2017. PMID: 28104760 Free PMC article. No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB. Heart disease and stroke statistics--2015 update: A report from the american heart association. Circulation. 2015;131:e29–322. - PubMed
-
- CDC. High blood pressure facts. 2016 cdc.Gov.
-
- Yoon SS, Carroll MD, Fryar CD. Hypertension prevalence and control among adults: United states, 2011–2014. NCHS Data Brief. 2015:1–8. - PubMed
-
- Modolo R, de Faria AP, Sabbatini AR, Barbaro NR, Ritter AM, Moreno H. Refractory and resistant hypertension: Characteristics and differences observed in a specialized clinic. J Am Soc Hypertens. 2015;9:397–402. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
