

Arterial and Cellular Inflammation in Patients with CKD
- PMID: 27799487
- PMCID: PMC5373444
- DOI: 10.1681/ASN.2016030317
Arterial and Cellular Inflammation in Patients with CKD
Abstract
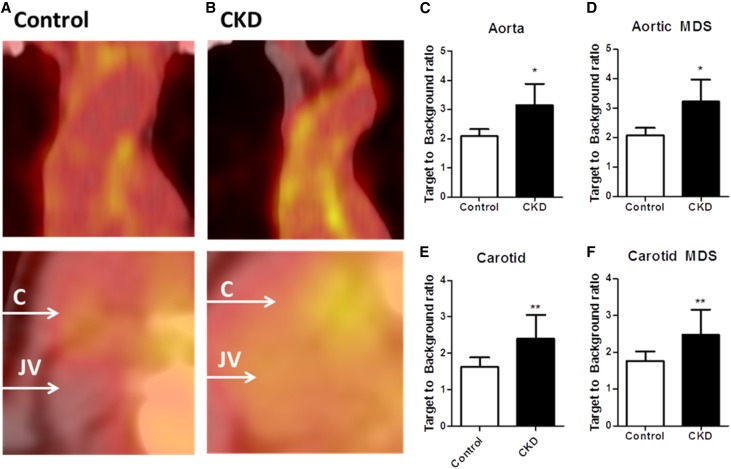
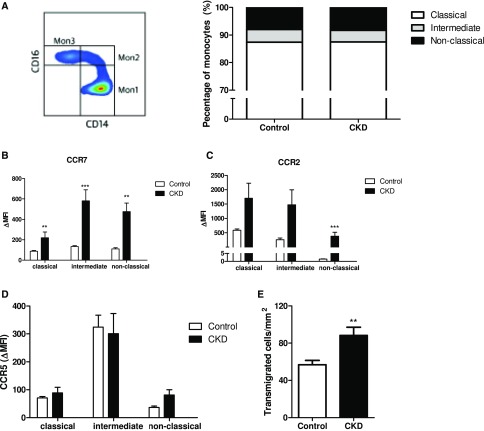
CKD associates with a 1.5- to 3.5-fold increased risk for cardiovascular disease. Both diseases are characterized by increased inflammation, and in patients with CKD, elevated C-reactive protein level predicts cardiovascular risk. In addition to systemic inflammation, local arterial inflammation, driven by monocyte-derived macrophages, predicts future cardiovascular events in the general population. We hypothesized that subjects with CKD have increased arterial and cellular inflammation, reflected by 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography computed tomography (PET/CT) of the arterial wall and a migratory phenotype of monocytes. We assessed 18F-FDG uptake in the arterial wall in 14 patients with CKD (mean±SD age: 59±5 years, mean±SD eGFR: 37±12 ml/min per 1.73 m2) but without cardiovascular diseases, diabetes, or inflammatory conditions and in 14 control subjects (mean age: 60±11 years, mean eGFR: 86±16 ml/min per 1.73 m2). Compared with controls, patients with CKD showed increased arterial inflammation, quantified as target-to-background ratio (TBR) in the aorta (TBRmax: CKD, 3.14±0.70 versus control, 2.12±0.27; P=0.001) and the carotid arteries (TBRmax: CKD, 2.45±0.65 versus control, 1.66±0.27; P<0.001). Characterization of circulating monocytes using flow cytometry revealed increased chemokine receptor expression and enhanced transendothelial migration capacity in patients with CKD compared with controls. In conclusion, this increased arterial wall inflammation, observed in patients with CKD but without overt atherosclerotic disease and with few traditional risk factors, may contribute to the increased cardiovascular risk associated with CKD. The concomitant elevation of monocyte activity may provide novel therapeutic targets for attenuating this inflammation and thereby preventing CKD-associated cardiovascular disease.
Keywords: Chronic inflammation; cardiovascular disease; chemokine receptor; chronic kidney disease.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH: Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med 164: 659–663, 2004 - PubMed
-
- Jha V, Garcia-Garcia G, Iseki K, Li Z, Naicker S, Plattner B, Saran R, Wang AY-M, Yang C-W: Chronic kidney disease: global dimension and perspectives. Lancet 382: 260–272, 2013 - PubMed
-
- Weiner DE, Tighiouart H, Elsayed EF, Griffith JL, Salem DN, Levey AS, Sarnak MJ: The Framingham predictive instrument in chronic kidney disease. J Am Coll Cardiol 50: 217–224, 2007 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
