

C-reactive protein in outpatients with acute exacerbation of COPD: its relationship with microbial etiology and severity
- PMID: 27799762
- PMCID: PMC5085274
- DOI: 10.2147/COPD.S117129
C-reactive protein in outpatients with acute exacerbation of COPD: its relationship with microbial etiology and severity
Abstract
Background: C-reactive protein (CRP) measurement has proven valuable for detecting exacerbations, but its usefulness in predicting etiology remains controversial. Likewise, its potential value as a marker of severity, which is well established in patients with pneumonia, remains unproven in chronic obstructive pulmonary disease (COPD) exacerbations.
Methods: A cohort study of 118 patients with severe COPD and acute infectious exacerbations were included and followed up over 1 year. Episodes of exacerbations meeting Anthonisen's criteria type I-II were evaluated, analyzing the etiology and inflammatory response as measured by CRP in blood.
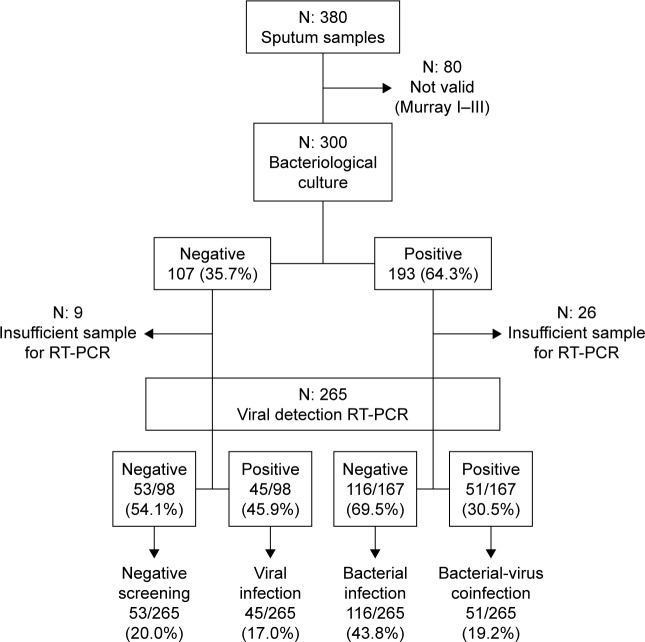
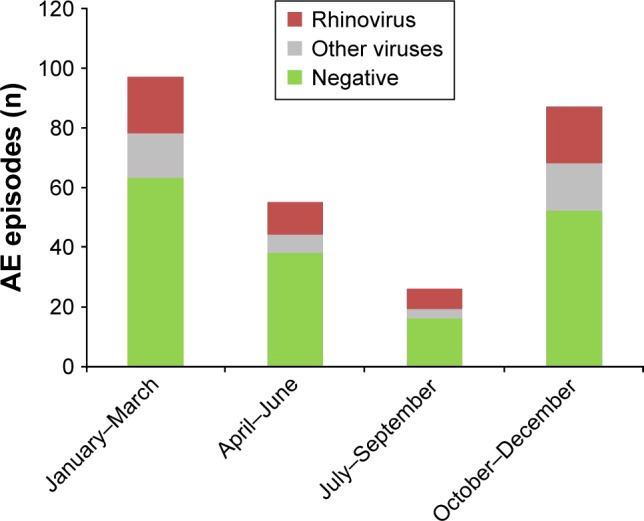
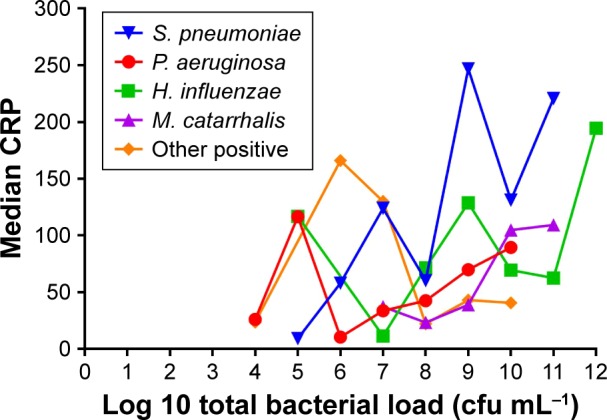
Results: A total of 380 episodes were recorded. Full microbiological analysis was available in 265 samples. Haemophilus influenzae was the most commonly isolated bacteria and rhinovirus the most common virus. Median CRP levels from the 265 episodes were higher in the cases with positive cultures for bacteria (58.30 mg/L, interquartile range [IQR] 21.0-28.2) than in episodes only positive for viruses (37.3 mg/L, IQR 18.6-79.1) and cases negative for any microorganism (36.4 mg/L, IQR 10.8-93.7) (P<0.014). H. influenzae and Streptococcus pneumoniae reached the highest CRP levels of 74.5 mg/L (IQR 23.9-167.9) and 74.1 mg/L (IQR 42.0-220.7), respectively. In the 380 exacerbations studied, 227 (~60%) were community-managed, while 153 (~40%) required hospital admission. In the multivariate analysis to assess the influence of inflammatory response on exacerbation severity, baseline hypercapnia (odds ratio [OR]: 2.70, 95% confidence interval [CI]: 1.46-4.9) and CRP levels >100 mg/L (OR: 4.23, 95% CI: 2.12-8.44) were independent predictors after adjustment for baseline characteristics.
Conclusion: CRP level was higher in bacterial infections, especially when H. influenzae and S. pneumoniae were isolated. CRP values >100 mg/L were associated with a fourfold increased risk of hospital admission. Therefore, CRP blood levels may be a useful biomarker in the management of exacerbations appearing in patients with severe disease.
Keywords: C-reactive protein; COPD exacerbations; hospital admission; viruses.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Hurst JR, Vestbo J, Anzueto A, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. - PubMed
-
- Miravitlles M, Anzueto A. Role of infection in exacerbations of chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2015;21(3):278–283. - PubMed
-
- Stockley RA, O’Brien C, Pye A, Hill SL. Relationship of sputum color to nature and outpatient management of acute exacerbations of COPD. Chest. 2000;117(6):1638–1645. - PubMed
-
- Miravitlles M, Kruesmann F, Haverstock D, Perroncel R, Choudhri SH, Arvis P. Sputum colour and bacteria in chronic bronchitis exacerbations: a pooled analysis. Eur Respir J. 2012;39(6):1354–1360. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
