

Intraoperative Fluorescence Imaging for Personalized Brain Tumor Resection: Current State and Future Directions
- PMID: 27800481
- PMCID: PMC5066076
- DOI: 10.3389/fsurg.2016.00055
Intraoperative Fluorescence Imaging for Personalized Brain Tumor Resection: Current State and Future Directions
Abstract
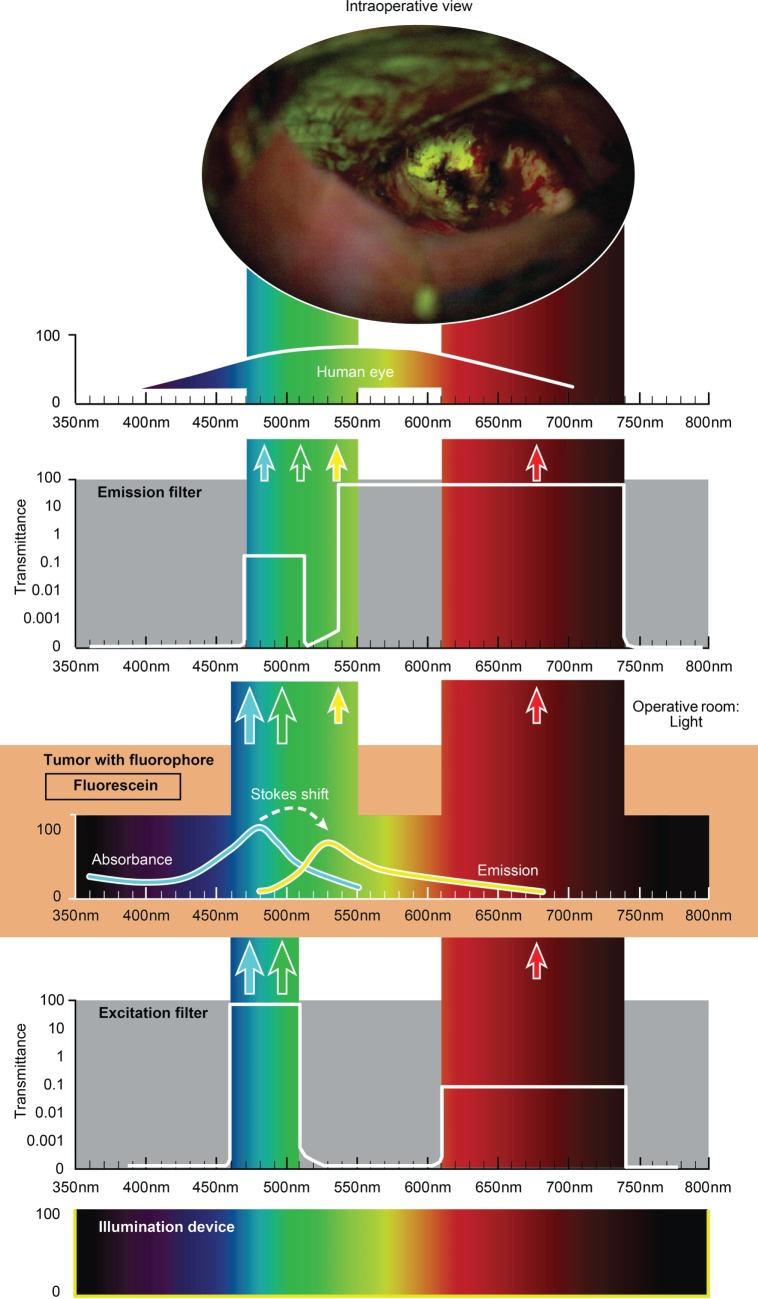
Introduction: Fluorescence-guided surgery is one of the rapidly emerging methods of surgical "theranostics." In this review, we summarize current fluorescence techniques used in neurosurgical practice for brain tumor patients as well as future applications of recent laboratory and translational studies.
Methods: Review of the literature.
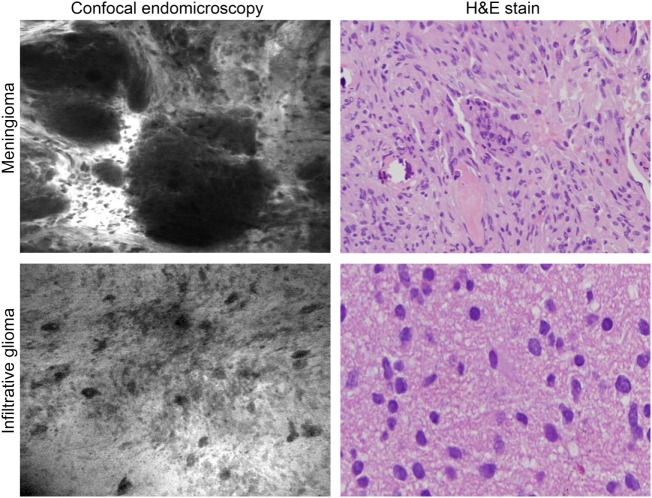
Results: A wide spectrum of fluorophores that have been tested for brain surgery is reviewed. Beginning with a fluorescein sodium application in 1948 by Moore, fluorescence-guided brain tumor surgery is either routinely applied in some centers or is under active study in clinical trials. Besides the trinity of commonly used drugs (fluorescein sodium, 5-aminolevulinic acid, and indocyanine green), less studied fluorescent stains, such as tetracyclines, cancer-selective alkylphosphocholine analogs, cresyl violet, acridine orange, and acriflavine, can be used for rapid tumor detection and pathological tissue examination. Other emerging agents, such as activity-based probes and targeted molecular probes that can provide biomolecular specificity for surgical visualization and treatment, are reviewed. Furthermore, we review available engineering and optical solutions for fluorescent surgical visualization. Instruments for fluorescent-guided surgery are divided into wide-field imaging systems and hand-held probes. Recent advancements in quantitative fluorescence-guided surgery are discussed.
Conclusion: We are standing on the threshold of the era of marker-assisted tumor management. Innovations in the fields of surgical optics, computer image analysis, and molecular bioengineering are advancing fluorescence-guided tumor resection paradigms, leading to cell-level approaches to visualization and resection of brain tumors.
Keywords: 5-ALA; ICG; confocal; endomicroscopy; fluorescein; fluorescence-guided surgery; fluorescent probe; glioma.
Figures




Similar articles
-
Fluorescence-Guided Surgery: A Review on Timing and Use in Brain Tumor Surgery.Front Neurol. 2021 Jun 16;12:682151. doi: 10.3389/fneur.2021.682151. eCollection 2021. Front Neurol. 2021. PMID: 34220688 Free PMC article. Review.
-
5-aminolevulinic acid, fluorescein sodium, and indocyanine green for glioma margin detection: analysis of operating wide-field and confocal microscopy in glioma models of various grades.Front Oncol. 2023 May 23;13:1156812. doi: 10.3389/fonc.2023.1156812. eCollection 2023. Front Oncol. 2023. PMID: 37287908 Free PMC article.
-
Use of optical fluorescence agents during surgery for pituitary adenomas: current state of the field.J Neurooncol. 2019 Feb;141(3):585-593. doi: 10.1007/s11060-018-03062-2. Epub 2018 Dec 6. J Neurooncol. 2019. PMID: 30523607 Free PMC article.
-
Probe-based three-dimensional confocal laser endomicroscopy of brain tumors: technical note.Cancer Manag Res. 2018 Aug 30;10:3109-3123. doi: 10.2147/CMAR.S165980. eCollection 2018. Cancer Manag Res. 2018. PMID: 30214304 Free PMC article.
-
Intraoperative fluorescence-guided resection of high-grade gliomas: a comparison of the present techniques and evolution of future strategies.World Neurosurg. 2014 Jul-Aug;82(1-2):175-85. doi: 10.1016/j.wneu.2013.06.014. Epub 2013 Jul 9. World Neurosurg. 2014. PMID: 23851210 Review.
Cited by
-
Clinical Benefits of Combining Different Visualization Modalities in Neurosurgery.Front Surg. 2019 Oct 1;6:56. doi: 10.3389/fsurg.2019.00056. eCollection 2019. Front Surg. 2019. PMID: 31632980 Free PMC article.
-
Redosing of Fluorescein Sodium Improves Image Interpretation During Intraoperative Ex Vivo Confocal Laser Endomicroscopy of Brain Tumors.Front Oncol. 2021 Sep 30;11:668661. doi: 10.3389/fonc.2021.668661. eCollection 2021. Front Oncol. 2021. PMID: 34660258 Free PMC article.
-
A Fluorescence-Based Wireless Capsule Endoscopy System for Detecting Colorectal Cancer.Cancers (Basel). 2020 Apr 6;12(4):890. doi: 10.3390/cancers12040890. Cancers (Basel). 2020. PMID: 32268557 Free PMC article.
-
Intraoperative in vivo confocal endomicroscopy of the glioma margin: performance assessment of image interpretation by neurosurgeon users.Front Oncol. 2024 May 22;14:1389608. doi: 10.3389/fonc.2024.1389608. eCollection 2024. Front Oncol. 2024. PMID: 38841162 Free PMC article.
-
Fluorine-18-Labeled Fluorescent Dyes for Dual-Mode Molecular Imaging.Molecules. 2020 Dec 21;25(24):6042. doi: 10.3390/molecules25246042. Molecules. 2020. PMID: 33371284 Free PMC article. Review.
References
-
- Sanai N, Berger MS. Glioma extent of resection and its impact on patient outcome. Neurosurgery (2008) 62(4):753–64; discussion 264–6.10.1227/01.neu.0000318159.21731.cf - DOI - PubMed
-
- Akeyson EW, McCutcheon IE. Management of benign and aggressive intracranial meningiomas. Oncology (Williston Park) (1996) 10(5):747–56; discussion 756–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases