

Upregulation of Soluble HLA-G in Chronic Left Ventricular Systolic Dysfunction
- PMID: 27800497
- PMCID: PMC5075317
- DOI: 10.1155/2016/8417190
Upregulation of Soluble HLA-G in Chronic Left Ventricular Systolic Dysfunction
Abstract
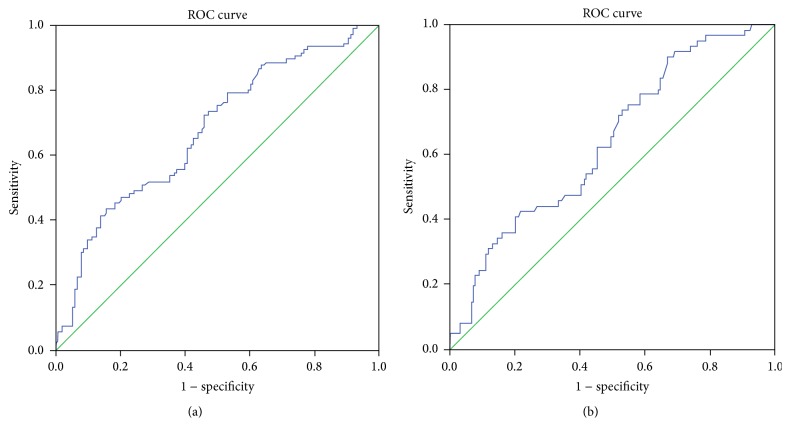
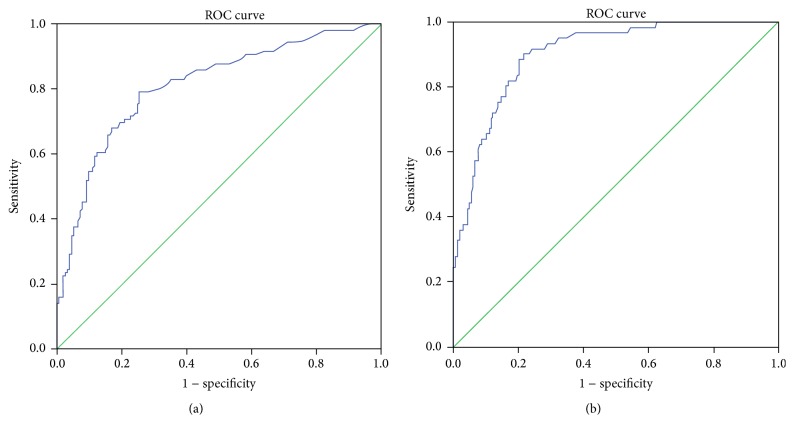
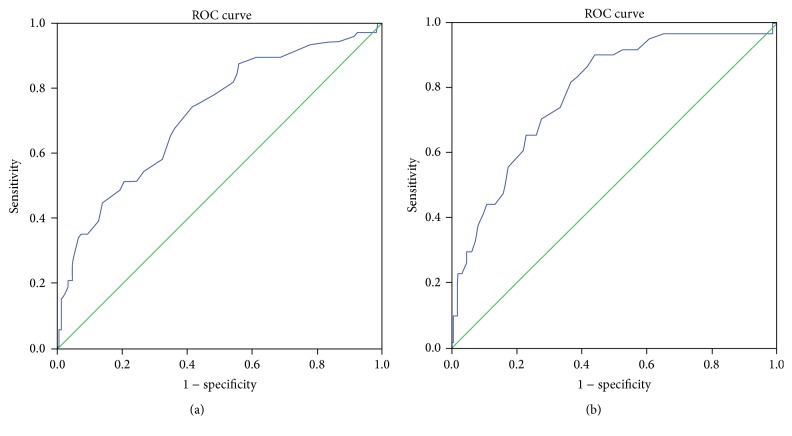
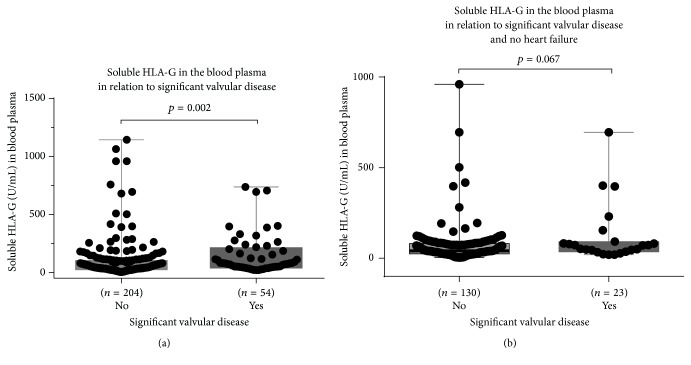
Left ventricular systolic dysfunction (LVSD) defined by ejection fraction (EF) <40% is common, serious but treatable, and correct diagnosis is the cornerstone of effective treatment. Biomarkers may help to diagnose LVSD and give insight into the pathophysiology. The immune system is activated in LVSD, and the immunomodulatory molecule human leukocyte antigen-G (HLA-G) may be involved. The primary aim was to measure soluble HLA-G (sHLA-G) in the blood in different stages of LVSD (<30% and 30-40%), in the midrange EF 40-50%, and in preserved EF ≥ 50% and to validate sHLA-G as a LVSD biomarker. The secondary aim was to examine associations between HLA-G gene polymorphisms influencing expression levels and LVSD. The 260 study participants were ≥75 years old, many with risk factors for heart disease or with known heart disease. Soluble HLA-G was significantly and uniformly higher in the groups with EF < 50% (<30, 30-40, and 40-50%) compared to EF > 50% (p < 0.0001). N-terminal fragment-pro-B-type natriuretic peptide (NT-proBNP) and uric acid values were inversely related to EF. According to Receiver Operating Characteristic (ROC) curves NT-proBNP outperformed both sHLA-G and uric acid as biomarkers of LVSD. Soluble HLA-G in blood plasma was elevated in LVSD regardless of EF. A novel finding was that a combined 14 bp ins-del/+3142 SNP HLA-G haplotype was associated with EF < 40%.
Figures

Similar articles
-
Head to head comparison of N-terminal pro-B-type natriuretic peptide and B-type natriuretic peptide in patients with/without left ventricular systolic dysfunction.Clin Biochem. 2006 Jun;39(6):640-5. doi: 10.1016/j.clinbiochem.2006.01.021. Epub 2006 Mar 3. Clin Biochem. 2006. PMID: 16516185
-
Pro-brain natriuretic peptide plasma levels, left ventricular dimensions and ejection fraction in acute dyspnoea.J Coll Physicians Surg Pak. 2012 Dec;22(12):751-5. J Coll Physicians Surg Pak. 2012. PMID: 23217478
-
Community screening for left ventricular systolic dysfunction using plasma and urinary natriuretic peptides.J Am Coll Cardiol. 2005 Apr 5;45(7):1043-50. doi: 10.1016/j.jacc.2004.12.058. J Am Coll Cardiol. 2005. PMID: 15808762
-
Diagnostic accuracy of natriuretic peptide screening for left ventricular systolic dysfunction in the community: systematic review and meta-analysis.ESC Heart Fail. 2023 Jun;10(3):1643-1655. doi: 10.1002/ehf2.14314. Epub 2023 Feb 13. ESC Heart Fail. 2023. PMID: 36785511 Free PMC article.
-
Association of parental HLA-G polymorphisms with soluble HLA-G expressions and their roles on recurrent implantation failure: A systematic review and meta-analysis.Front Immunol. 2022 Dec 1;13:988370. doi: 10.3389/fimmu.2022.988370. eCollection 2022. Front Immunol. 2022. PMID: 36532068 Free PMC article.
Cited by
-
Integrated analysis of DNA methylation profile of HLA-G gene and imaging in coronary heart disease: Pilot study.PLoS One. 2020 Aug 13;15(8):e0236951. doi: 10.1371/journal.pone.0236951. eCollection 2020. PLoS One. 2020. PMID: 32790754 Free PMC article.
-
Novel Cardiovascular Biomarkers Associated with Increased Cardiovascular Risk in Women With Prior Preeclampsia/HELLP Syndrome: A Narrative Review.Eur Cardiol. 2021 Sep 24;16:e36. doi: 10.15420/ecr.2021.21. eCollection 2021 Feb. Eur Cardiol. 2021. PMID: 34721670 Free PMC article. Review.
References
-
- Ponikowski P., Voors A. A., Anker S. D., et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. European Heart Journal. 2016;37(27):2129–2200. doi: 10.1093/eurheartj/ehw128. - DOI - PubMed
-
- Olesen L. L., Andersen A., Thaulow S. Hand-held echocardiography is useful for diagnosis of left systolic dysfunction in an elderly population. Danish Medical Journal. 2015;62(7):1–5.A5100 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
