

Treatment of Severe Adult Traumatic Brain Injury Using Bone Marrow Mononuclear Cells
- PMID: 27800660
- PMCID: PMC5367945
- DOI: 10.1002/stem.2538
Treatment of Severe Adult Traumatic Brain Injury Using Bone Marrow Mononuclear Cells
Abstract
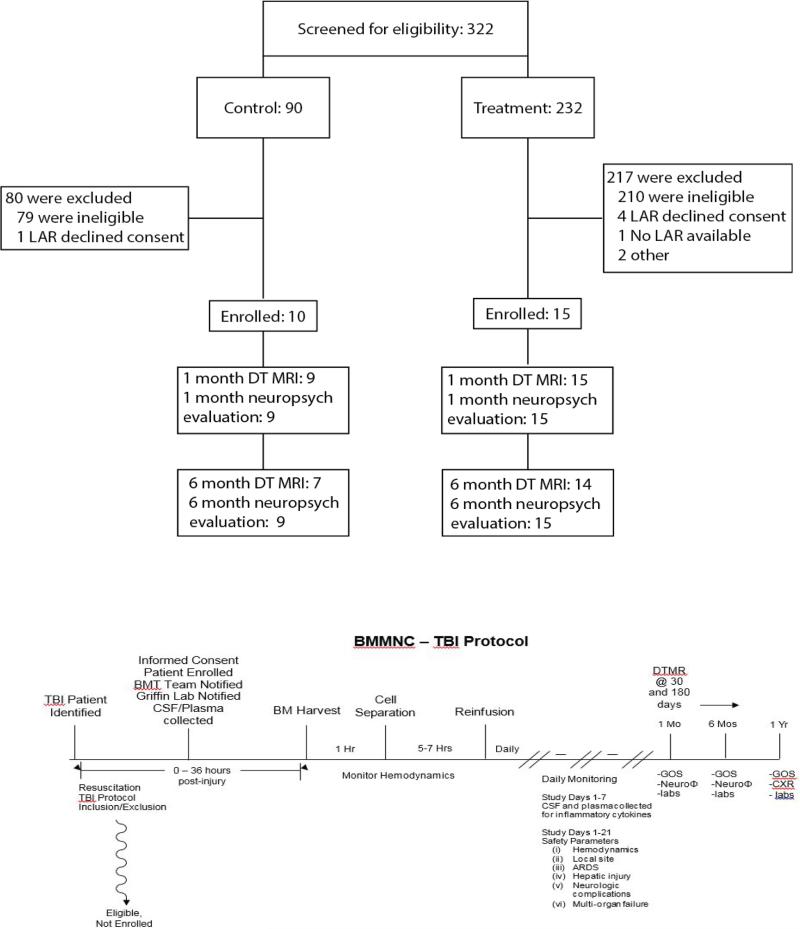
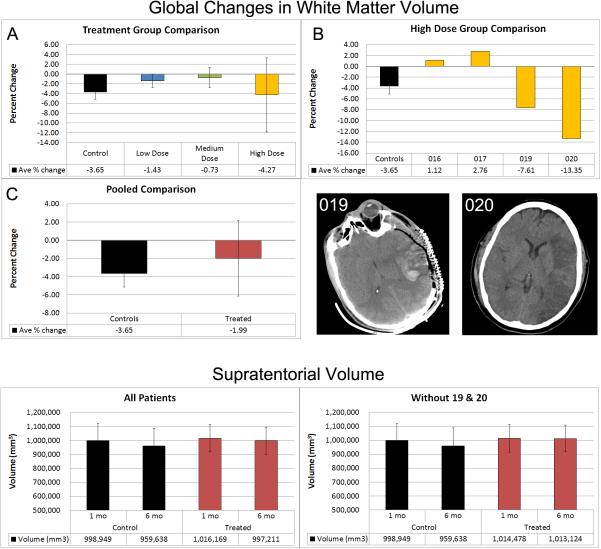
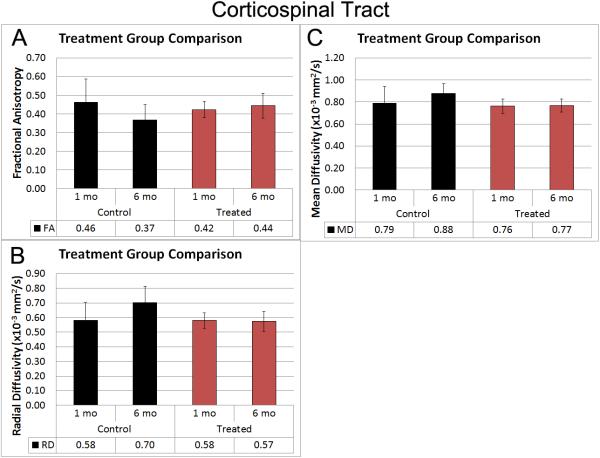
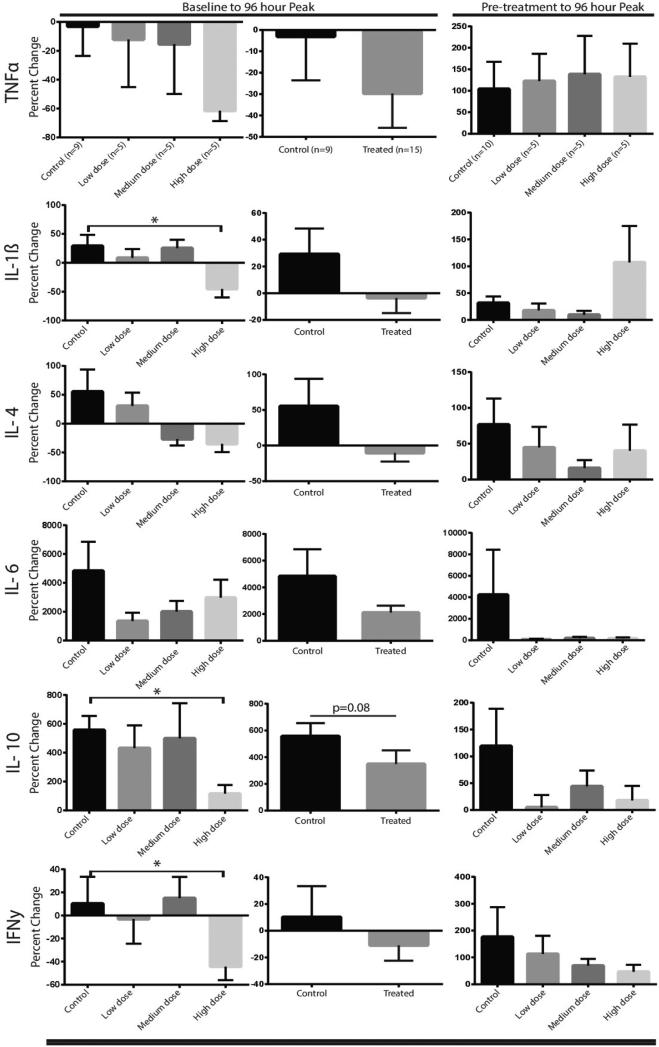
Preclinical studies using bone marrow derived cells to treat traumatic brain injury have demonstrated efficacy in terms of blood-brain barrier preservation, neurogenesis, and functional outcomes. Phase 1 clinical trials using bone marrow mononuclear cells infused intravenously in children with severe traumatic brain injury demonstrated safety and potentially a central nervous system structural preservation treatment effect. This study sought to confirm the safety, logistic feasibility, and potential treatment effect size of structural preservation/inflammatory biomarker mitigation in adults to guide Phase 2 clinical trial design. Adults with severe traumatic brain injury (Glasgow Coma Scale 5-8) and without signs of irreversible brain injury were evaluated for entry into the trial. A dose escalation format was performed in 25 patients: 5 controls, followed 5 patients in each dosing cohort (6, 9, 12 ×106 cells/kg body weight), then 5 more controls. Bone marrow harvest, cell processing to isolate the mononuclear fraction, and re-infusion occurred within 48 hours after injury. Patients were monitored for harvest-related hemodynamic changes, infusional toxicity, and adverse events. Outcome measures included magnetic resonance imaging-based measurements of supratentorial and corpus callosal volumes as well as diffusion tensor imaging-based measurements of fractional anisotropy and mean diffusivity of the corpus callosum and the corticospinal tract at the level of the brainstem at 1 month and 6 months postinjury. Functional and neurocognitive outcomes were measured and correlated with imaging data. Inflammatory cytokine arrays were measured in the plasma pretreatment, posttreatment, and at 1 and 6 month follow-up. There were no serious adverse events. There was a mild pulmonary toxicity of the highest dose that was not clinically significant. Despite the treatment group having greater injury severity, there was structural preservation of critical regions of interest that correlated with functional outcomes. Key inflammatory cytokines were downregulated. Treatment of severe, adult traumatic brain injury using an intravenously delivered autologous bone marrow mononuclear cell infusion is safe and logistically feasible. There appears to be a treatment signal as evidenced by central nervous system structural preservation, consistent with previous pediatric trial data. Inflammatory biomarkers are downregulated after cell infusion. Stem Cells 2016 Video Highlight: https://youtu.be/UiCCPIe-IaQ Stem Cells 2017;35:1065-1079.
Keywords: adult human bone marrow; adult stem cells; bone marrow stromal cells; cellular therapy; clinical trials; diffusion tensor imaging; traumatic brain injury.
© 2016 AlphaMed Press.
Figures

References
-
- Centers for Disease Control and Prevention . Report to Congress on Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation. National Center for Injury Prevention and Control; Division of Unintentional Injury Prevention; Atlanta, GA.: 2015.
-
- Kraus JF, McArthur DL. Epidemiologic aspects of brain injury. NEUROL CLIN. 1996;14:435–50. - PubMed
-
- Savitz SI, Cox CS., Jr. Concise review: Cell therapies for stroke and traumatic brain injury: Targeting microglia. Stem Cells. 2016;34:537–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
