

Dietary protein intake and chronic kidney disease
- PMID: 27801685
- PMCID: PMC5962279
- DOI: 10.1097/MCO.0000000000000342
Dietary protein intake and chronic kidney disease
Abstract
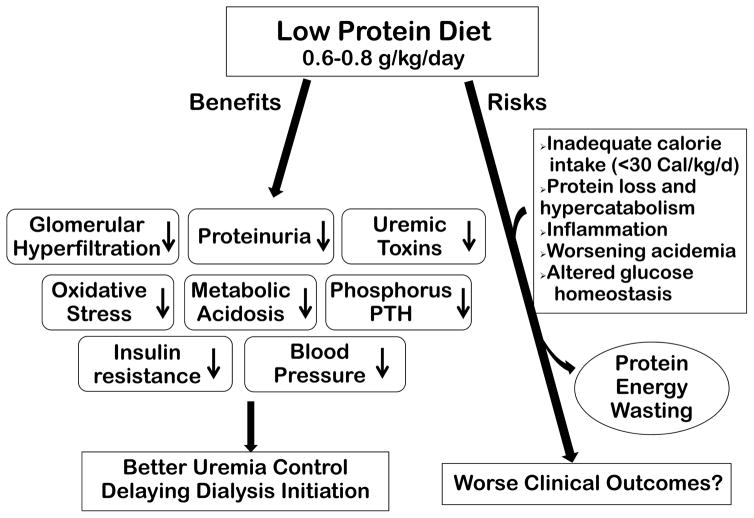
Purpose of review: High-protein intake may lead to increased intraglomerular pressure and glomerular hyperfiltration. This can cause damage to glomerular structure leading to or aggravating chronic kidney disease (CKD). Hence, a low-protein diet (LPD) of 0.6-0.8 g/kg/day is often recommended for the management of CKD. We reviewed the effect of protein intake on incidence and progression of CKD and the role of LPD in the CKD management.
Recent findings: Actual dietary protein consumption in CKD patients remains substantially higher than the recommendations for LPD. Notwithstanding the inconclusive results of the 'Modification of Diet in Renal Disease' (MDRD) study, the largest randomized controlled trial to examine protein restriction in CKD, several prior and subsequent studies and meta-analyses appear to support the role of LPD on retarding progression of CKD and delaying initiation of maintenance dialysis therapy. LPD can also be used to control metabolic derangements in CKD. Supplemented LPD with essential amino acids or their ketoanalogs may be used for incremental transition to dialysis especially on nondialysis days. The LPD management in lieu of dialysis therapy can reduce costs, enhance psychological adaptation, and preserve residual renal function upon transition to dialysis. Adherence and adequate protein and energy intake should be ensured to avoid protein-energy wasting.
Summary: A balanced and individualized dietary approach based on LPD should be elaborated with periodic dietitian counseling and surveillance to optimize management of CKD, to assure adequate protein and energy intake, and to avoid or correct protein-energy wasting.
Conflict of interest statement
Dr. K. Kalantar-Zadeh has received honoraria and/or support from Abbott, Abbvie, Alexion, Amgen, ASN (American Society of Nephrology), Astra-Zeneca, Aveo, Chugai, DaVita, Fresenius, Genentech, Haymarket Media, Hofstra Medical School, IFKF (International Federation of Kidney Foundations), ISH (International Society of Hemodialysis), International Society of Renal Nutrition & Metabolism (ISRNM), JSDT (Japanese Society of Dialysis Therapy), Hospira, Kabi, Keryx, Novartis, NIH (National Institutes of Health), NKF (National Kidney Foundations), Pfizer, Relypsa, Resverlogix, Sandoz, Sanofi, Shire, Vifor, UpToDate, ZS-Pharma.
Figures

References
-
- Kalantar-Zadeh K, Moore LW, Tortorici AR, et al. North American experience with Low protein diet for Non-dialysis-dependent chronic kidney disease. BMC Nephrol. 2016;17:90. This review paper evaluated the current status of diet pattern in North America, impact of current consumption of protein, role of low protein diet in CKD patients, and the obstacles for implementation of low protein diet in North America. - PMC - PubMed
-
- Fouque D, Aparicio M. Eleven reasons to control the protein intake of patients with chronic kidney disease. Nat Clin Pract Nephrol. 2007;3:383–392. - PubMed
-
- Larsen RN, Mann NJ, Maclean E, et al. The effect of high-protein, low-carbohydrate diets in the treatment of type 2 diabetes: a 12 month randomised controlled trial. Diabetologia. 2011;54:731–740. - PubMed
-
- Krebs JD, Elley CR, Parry-Strong A, et al. The Diabetes Excess Weight Loss (DEWL) Trial: a randomised controlled trial of high-protein versus high-carbohydrate diets over 2 years in type 2 diabetes. Diabetologia. 2012;55:905–914. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
