

Prediction of Pneumonia in Acute Stroke Patients Using Tongue Pressure Measurements
- PMID: 27802333
- PMCID: PMC5089549
- DOI: 10.1371/journal.pone.0165837
Prediction of Pneumonia in Acute Stroke Patients Using Tongue Pressure Measurements
Expression of concern in
-
Expression of Concern: Prediction of Pneumonia in Acute Stroke Patients Using Tongue Pressure Measurements.PLoS One. 2023 Jan 11;18(1):e0279804. doi: 10.1371/journal.pone.0279804. eCollection 2023. PLoS One. 2023. PMID: 36630346 Free PMC article. No abstract available.
Abstract
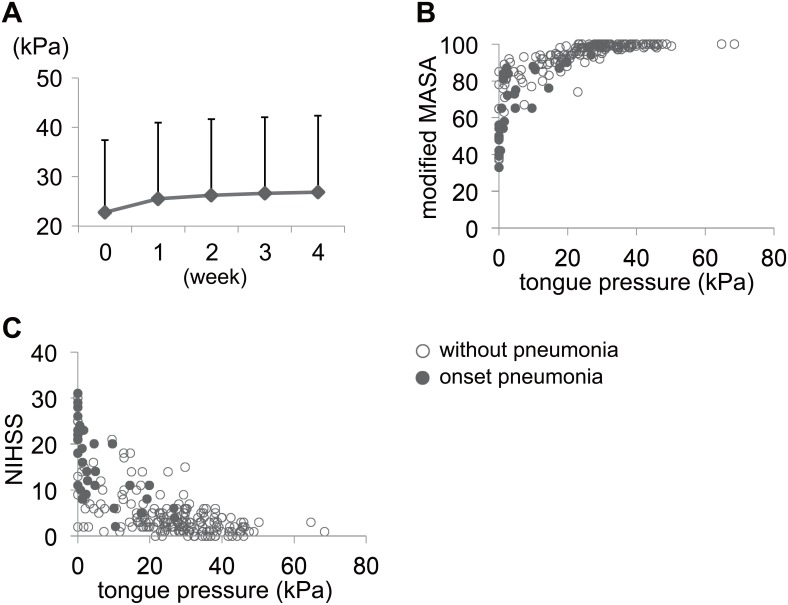
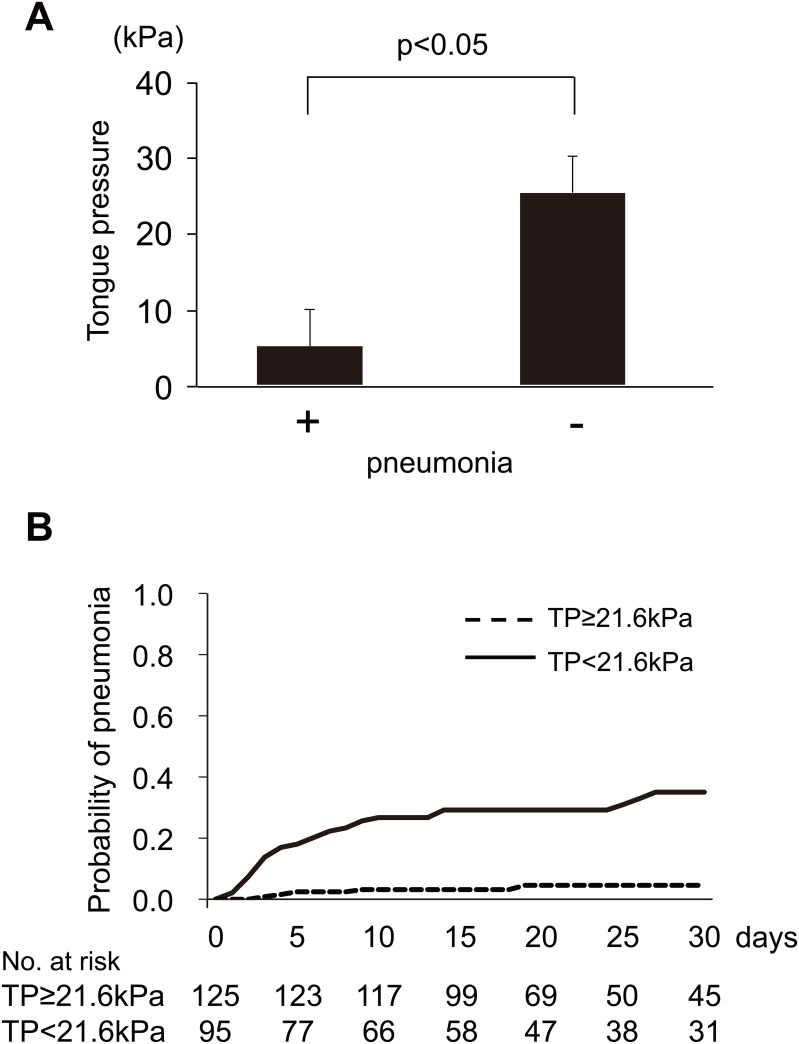
Swallowing dysfunction caused by stroke is a risk factor for aspiration pneumonia. Tongue pressure measurement is a simple and noninvasive method for evaluating swallowing dysfunction. We have hypothesized that low tongue pressure may be able to predict pneumonia occurrence in acute stroke patients. Tongue pressure was measured using balloon-type equipment in 220 acute stroke patients. The modified Mann Assessment of Swallowing Ability (MASA) score was evaluated independently on the same day. Tongue pressure was measured every week thereafter. An improvement in tongue pressure was observed within the first 2 weeks. Receiver operating curve analysis was performed to determine the ability of tongue pressure to predict modified MASA score <95, which suggests swallowing dysfunction. The optimal cutoff for tongue pressure was 21.6 kPa (χ2 = 45.82, p<0.001, sensitivity 95.9%, specificity 91.8%, area under the curve = 0.97). The tongue pressure was significantly lower in patients with pneumonia than in those without pneumonia. Using a Cox proportional hazard model for pneumonia onset with a cutoff tongue pressure value of 21.6 kPa and adjustment for age, sex, and National Institutes of Health Stroke Scale score at admission, the tongue pressure had additional predictive power for pneumonia onset (hazard ratio, 7.95; 95% confidence interval, 2.09 to 52.11; p = 0.0013). In the group with low tongue pressure, 27 of 95 patients showed improvement of tongue pressure within 2 weeks. Pneumonia occurred frequently in patients without improvement of tongue pressure, but not in patients with improvement (31/68 and 2/27, p<0.001). Tongue pressure is a sensitive indicator for predicting pneumonia occurrence in acute stroke patients.
Conflict of interest statement
MM reports grants from Mochida Pharmaceutical Co., LTD., Otsuka Pharmaceutical, and Daiichi Sankyo Co., LTD. and honoraria from Sanofi K.K., Bayer Health Care, Otsuka Pharmaceutical, Daiichi Sankyo Co., LTD., Boehringer Ingelheim, and Sumitomo Dainippon Pharma Co., LTD., which are outside the submitted work. NH reports an honorarium from Mochida Pharmaceutical Co., LTD., which is outside the submitted work. The other authors have declared that no competing interests exist. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- 1. Hinds NP, Wiles CM (1998) Assessment of swallowing and referral to speech and language therapists in acute stroke. QJM 91: 829–835. - PubMed
-
- Smithard DG, O'Neill PA, Parks C, Morris J (1996) Complications and outcome after acute stroke. Does dysphagia matter? Stroke 27: 1200–1204. - PubMed
-
- Shaker R, Cook IJ, Dodds WJ, Hogan WJ (1988) Pressure-flow dynamics of the oral phase of swallowing. Dysphagia 3: 79–84. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
