

Surgeon-performed point-of-care ultrasound in severe eye trauma: Report of two cases
- PMID: 27803918
- PMCID: PMC5067499
- DOI: 10.12998/wjcc.v4.i10.344
Surgeon-performed point-of-care ultrasound in severe eye trauma: Report of two cases
Abstract
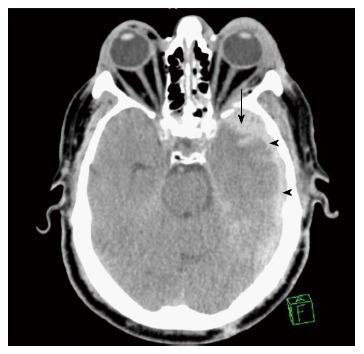
The indications of point-of-care ultrasound (POCUS) in the management of multiple trauma patients have been expanding. Although computed tomography (CT) scan of the orbit remains the gold standard for imaging orbital trauma, ultrasound is a quick, safe, and portable tool that can be performed bedside. Here we report two patients who had severe eye injuries with major visual impairment where surgeon-performed POCUS was very useful. One had a foreign body injury while the other had blunt trauma. POCUS was done using a linear probe under sterile conditions with minimum pressure on the eyes. Ultrasound showed a foreign body at the back of the left eye globe touching the eye globe in the first patient, and was normal in the second patient. Workup using CT scan, fundsocopy, optical coherence tomography, and magnetic resonance imaging of the orbits confirmed these findings. The first patient had vitreous and sub retinal haemorrhage and a full thickness macular hole of the left eye, while the second had traumatic optic neuropathy. POCUS gave accurate information concerning severe eye injuries. Trauma surgeons and emergency physicians should be trained in performing ocular ultrasound for eye injuries.
Keywords: Eye; Injury; Point-of-care; Trauma; Ultrasound.
Conflict of interest statement
Conflict-of-interest statement: None declared by all authors.
Figures










References
-
- Mohammad A, Hefny AF, Abu-Zidan FM. Focused Assessment Sonography for Trauma (FAST) training: a systematic review. World J Surg. 2014;38:1009–1018. - PubMed
-
- Dunkin JM, Crum AV, Swanger RS, Bokhari SA. Globe trauma. Semin Ultrasound CT MR. 2011;32:51–56. - PubMed
-
- Poon A, McCluskey PJ, Hill DA. Eye injuries in patients with major trauma. J Trauma. 1999;46:494–499. - PubMed
-
- Sung EK, Nadgir RN, Fujita A, Siegel C, Ghafouri RH, Traband A, Sakai O. Injuries of the globe: what can the radiologist offer? Radiographics. 2014;34:764–776. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
