

Increased anatomic severity predicts outcomes: Validation of the American Association for the Surgery of Trauma's Emergency General Surgery score in appendicitis
- PMID: 27805996
- PMCID: PMC5337403
- DOI: 10.1097/TA.0000000000001274
Increased anatomic severity predicts outcomes: Validation of the American Association for the Surgery of Trauma's Emergency General Surgery score in appendicitis
Abstract
Background: Determination and reporting of disease severity in emergency general surgery lacks standardization. Recently, the American Association for the Surgery of Trauma (AAST) proposed an anatomic severity grading system. We aimed to validate this system in patients with appendicitis and determine if cross-sectional imaging correlates with disease severity at operation.
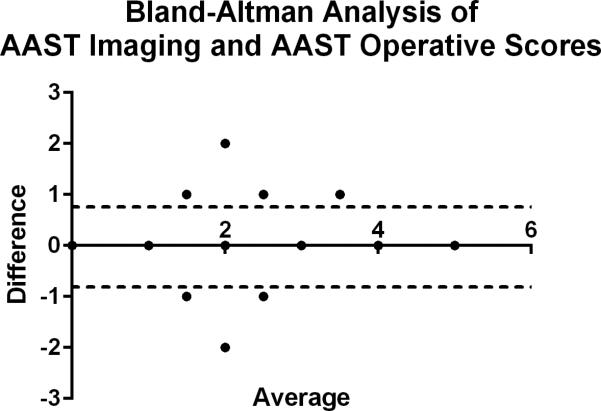
Methods: Patients 18 years or older undergoing treatment for acute appendicitis between 2013 and 2015 were identified. Baseline demographics, procedure types were recorded, and AAST grades were assigned based on intraoperative and radiologic findings. Outcomes including length of stay, 30-day mortality, and complications based on Clavien-Dindo categories and National Surgical Quality Improvement Program variables. Summary statistical univariate, nominal logistic, and standard least squares analyses were performed comparing AAST grade with key outcomes. Bland-Altman analysis compared operative findings with preoperative cross-sectional imaging to compare assigning grades.
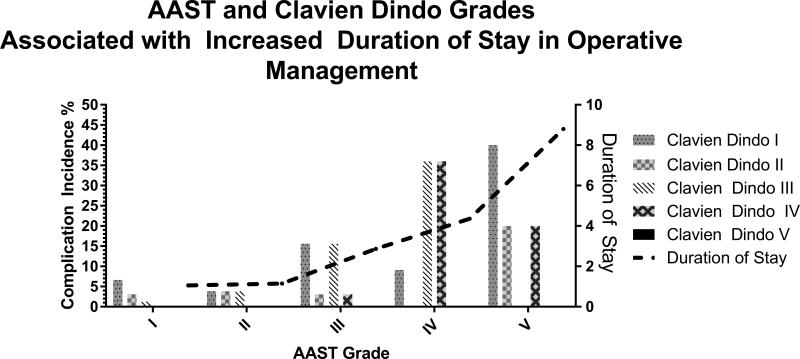
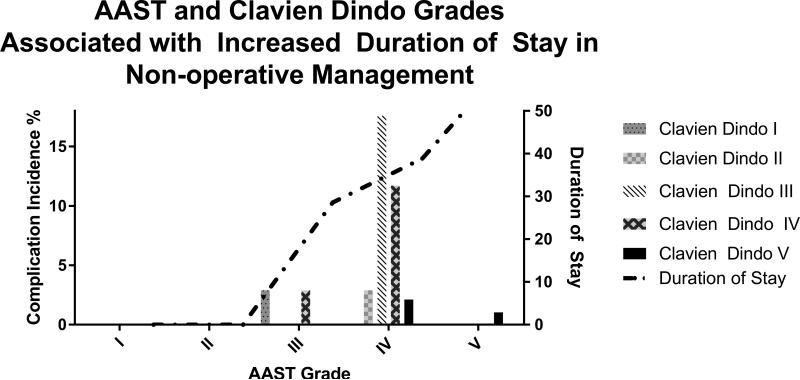
Results: Three hundred thirty-four patients with mean (±SD) age of 39.3 years (±16.5) were included (53% men), and all patients had cross-sectional imaging. Two hundred ninety-nine underwent appendectomy, and 85% completed laparoscopic. Thirty-day mortality rate was 0.9%, complication rate was 21%. Increased (median [interquartile range, IQR]) AAST grade was recorded in patients with complications (2 [1-4]) compared with those without (1 [1-1], p = 0.001). For operative management, (median [IQR]) AAST grades were significantly associated with procedure type: laparoscopic (1 [1-1]), open (4 [2-5]), conversion to open (3 [1-4], p = 0.001). Increased (median [IQR]) AAST grades were significantly associated in nonoperative management: patients having a complication had a higher median AAST grade (4 [3-5]) compared with those without (3 [2-3], p = 0.001). Bland-Altman analysis comparing AAST grade and cross-sectional imaging demonstrated no difference (-0.02 ± 0.02; p = 0.2; coefficient of repeatability 0.9).
Conclusions: The AAST grading system is valid in our population. Increased AAST grade is associated with open procedures, complications, and length of stay. The AAST emergency general surgery grade determined by preoperative imaging strongly correlated to operative findings.
Level of evidence: Epidemiologic/prognostic study, level III.
Figures
References
-
- Neary WD, Prytherch D, Foy C, Hearter BP, Earnshaw JJ. Comparison of different methods of risk stratification in urgent and emergency surgery. Br J Surg. 2007;94:1300–1305. - PubMed
-
- Masoomi H, Nguyen NT, Dolich MO, Mills S, Carmichael JC, Stamos MJ. Laparoscopic appendectomy trends and outcomes in the United States: Data from the Nationwide Inpatient Sample (NIS), 2004-2011. Am Surg. 2014;80:1074–1077. - PubMed
-
- Alvarado A. A practical score for the early diagnosis of appendicitis. Ann Emerg. 1985;15(5):557–564. - PubMed
-
- Doria AS, Moineddin R, Kellenberger CJ, Epelman M, Beyene J, Schuh S, Babyn PS, Dick PT. US or CT for Diagnosis of Appendicitis in Children and Adults? A Meta-Analysis. Radiology. 2006;241:83–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
