

Association of Neurocognition With Transition to Psychosis: Baseline Functioning in the Second Phase of the North American Prodrome Longitudinal Study
- PMID: 27806157
- PMCID: PMC5511703
- DOI: 10.1001/jamapsychiatry.2016.2479
Association of Neurocognition With Transition to Psychosis: Baseline Functioning in the Second Phase of the North American Prodrome Longitudinal Study
Abstract
Importance: Neurocognition is a central characteristic of schizophrenia and other psychotic disorders. Identifying the pattern and severity of neurocognitive functioning during the "near-psychotic," clinical high-risk (CHR) state of psychosis is necessary to develop accurate risk factors for psychosis and more effective and potentially preventive treatments.
Objectives: To identify core neurocognitive dysfunctions associated with the CHR phase, measure the ability of neurocognitive tests to predict transition to psychosis, and determine if neurocognitive deficits are robust or explained by potential confounders.
Design, setting, and participants: In this case-control study across 8 sites, baseline neurocognitive data were collected from January 2009 to April 2013 in the second phase of the North American Prodrome Longitudinal Study (NAPLS 2). The dates of analysis were August 2015 to August 2016. The setting was a consortium of 8 university-based, outpatient programs studying the psychosis prodrome in North America. Participants were 264 healthy controls (HCs) and 689 CHR individuals, aged 12 to 35 years.
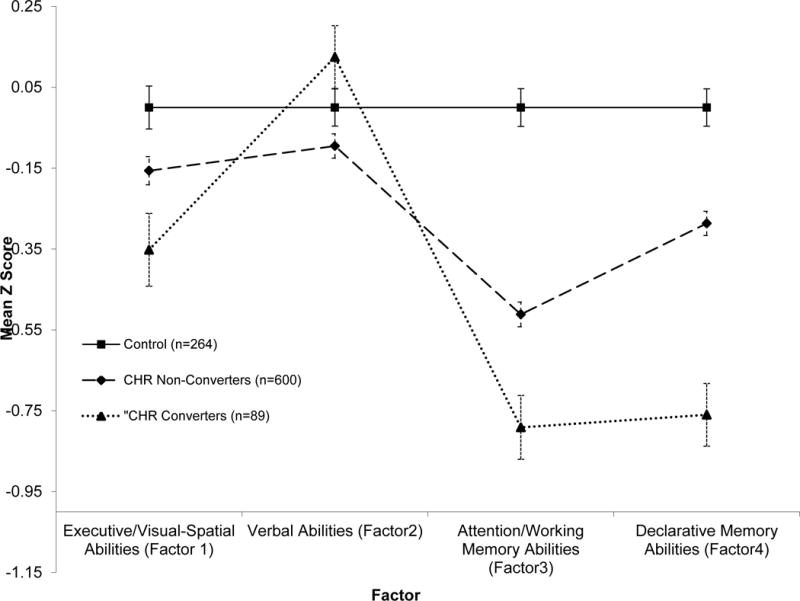
Main outcomes and measures: Neurocognitive associations with transition to psychosis and effects of medication on neurocognition. Nineteen neuropsychological tests and 4 factors derived from factor analysis were used: executive and visuospatial abilities, verbal abilities, attention and working memory abilities, and declarative memory abilities.
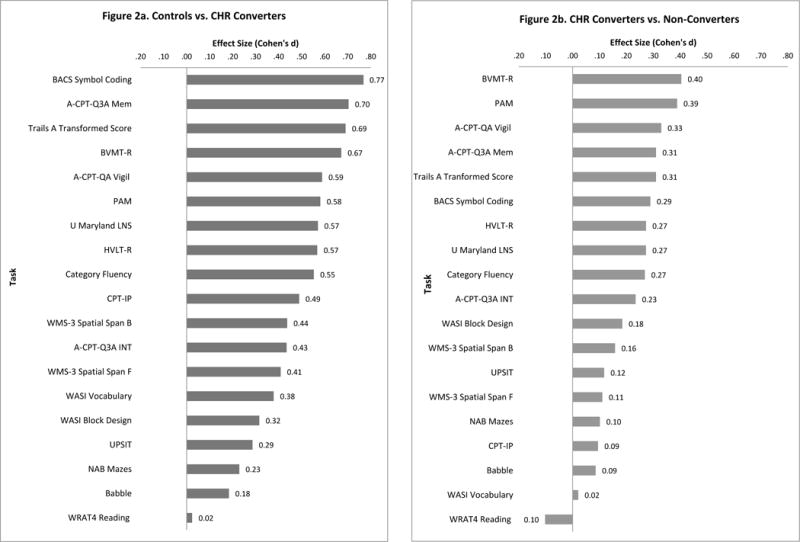
Results: This study included 264 HCs (137 male and 127 female) and 689 CHR participants (398 male and 291 female). In the HCs, 145 (54.9%) were white and 119 (45.1%) were not, whereas 397 CHR participants (57.6%) were white and 291 (42.3%) were not. In the HCs, 45 (17%) were of Hispanic origin, whereas 127 CHR participants (18.4%) were of Hispanic origin. The CHR individuals were significantly impaired compared with HCs on attention and working memory abilities and declarative memory abilities. The CHR converters had large deficits in attention and working memory abilities and declarative memory abilities (Cohen d, approximately 0.80) compared with controls and performed significantly worse on these dimensions than nonconverters (Cohen d, 0.28 and 0.48, respectively). These results were not accounted for by general cognitive ability or medications. In Cox proportional hazards regression, time to conversion in those who transitioned to psychosis was significantly predicted by high verbal (premorbid) abilities (β = 0.40; hazard ratio [HR], 1.48; 95% CI, 1.08-2.04; P = .02), impaired declarative memory abilities (β = -0.87; HR, 0.42; 95% CI, 0.31-0.56; P < .001), age (β = -0.10; HR, 0.90; 95% CI, 0.84-0.97; P = .003), site, and a combined score of unusual thought content or delusional ideas and suspiciousness or persecutory ideas items (β = 0.44; HR, 1.56; 95% CI, 1.36-1.78; P < .001).
Conclusions and relevance: Neurocognitive impairment, especially in attention and working memory abilities and declarative memory abilities, is a robust characteristic of CHR participants, especially those who later develop psychosis. Interventions targeting the enhancement of neurocognitive functioning are warranted in this population.
Conflict of interest statement
Figures
Comment in
-
Challenges and Opportunities in Studies of Cognition in the Prodrome to Psychosis: No Detail Is Too Small.JAMA Psychiatry. 2016 Dec 1;73(12):1249-1250. doi: 10.1001/jamapsychiatry.2016.2655. JAMA Psychiatry. 2016. PMID: 27806154 No abstract available.
-
Open Wards in Psychiatric Clinics and Compulsory Psychiatric Admissions-Reply.JAMA Psychiatry. 2016 Dec 1;73(12):1293-1294. doi: 10.1001/jamapsychiatry.2016.2669. JAMA Psychiatry. 2016. PMID: 27829089 No abstract available.
References
-
- Mirsky AF. Neuropsychological bases of schizophrenia. Ann Rev Psychol. 1969;20:321–348. - PubMed
-
- Seidman LJ. Schizophrenia and brain dysfunction: an integration of recent neurodiagnostic findings. Psychol Bull. 1983;94(2):195–238. - PubMed
-
- Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry. 1996;153(3):321–330. - PubMed
-
- Heinrichs RW. The primacy of cognition in schizophrenia. Am Psychol. 2005;60(3):229–242. - PubMed
-
- Kahn RS, Keefe RS. Schizophrenia is a cognitive illness: time for a change in focus. JAMA Psychiatry. 2013;70(10):1107–1112. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 MH082022/MH/NIMH NIH HHS/United States
- U01 MH081984/MH/NIMH NIH HHS/United States
- R01 MH096027/MH/NIMH NIH HHS/United States
- U01 MH081902/MH/NIMH NIH HHS/United States
- S10 RR019307/RR/NCRR NIH HHS/United States
- P50 MH080272/MH/NIMH NIH HHS/United States
- P41 RR014075/RR/NCRR NIH HHS/United States
- U01 MH081988/MH/NIMH NIH HHS/United States
- M01 RR001032/RR/NCRR NIH HHS/United States
- P50 MH066286/MH/NIMH NIH HHS/United States
- U01 MH076989/MH/NIMH NIH HHS/United States
- K24 MH076191/MH/NIMH NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- S10 RR023043/RR/NCRR NIH HHS/United States
- R01 MH060720/MH/NIMH NIH HHS/United States
- U01 MH081928/MH/NIMH NIH HHS/United States
- S10 RR023401/RR/NCRR NIH HHS/United States
- U01 MH081857/MH/NIMH NIH HHS/United States
- U01 MH082004/MH/NIMH NIH HHS/United States
- U01 MH081944/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
