

Fulminant Myocarditis with Combination Immune Checkpoint Blockade
- PMID: 27806233
- PMCID: PMC5247797
- DOI: 10.1056/NEJMoa1609214
Fulminant Myocarditis with Combination Immune Checkpoint Blockade
Abstract
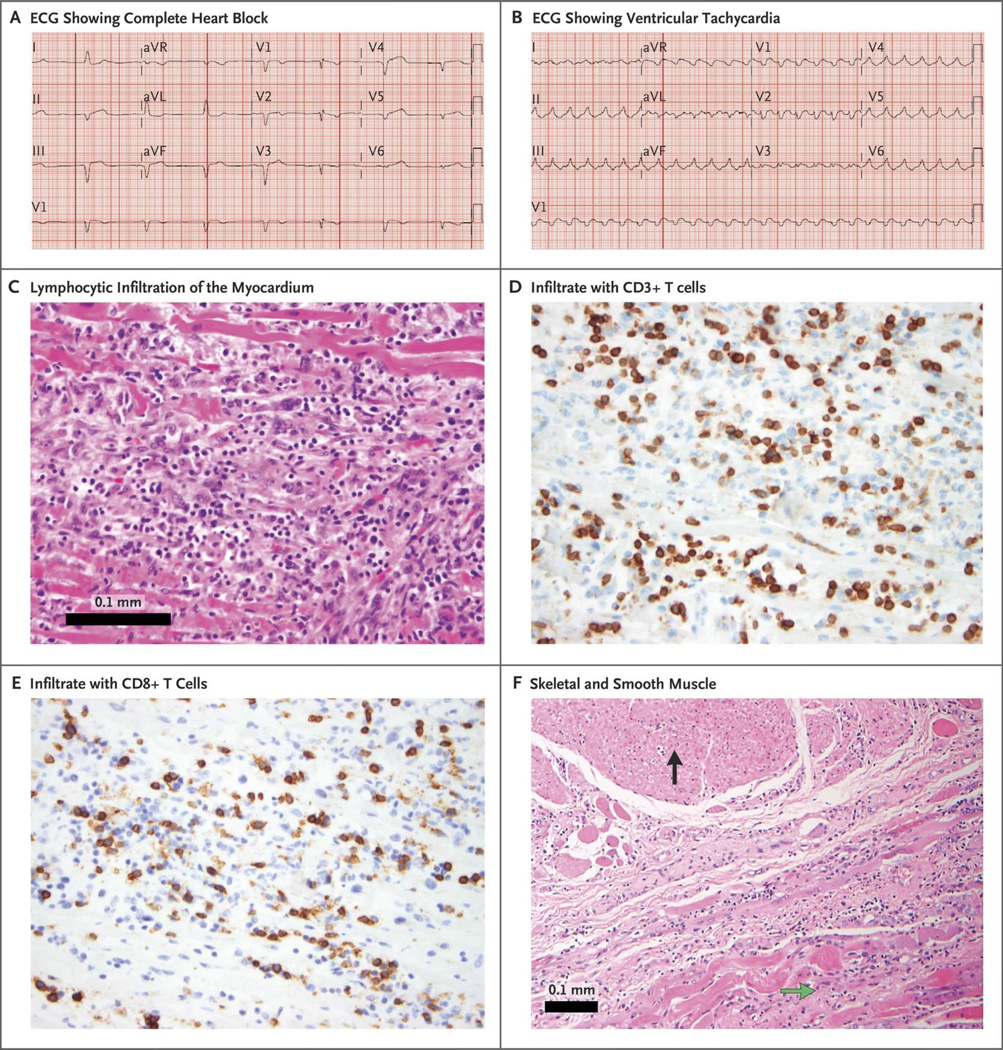
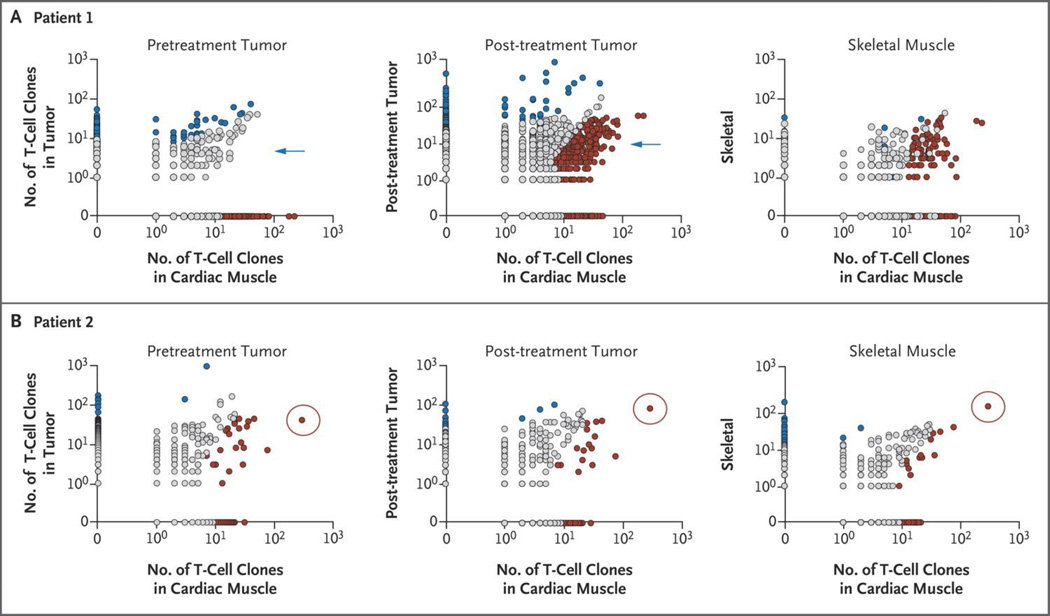
Immune checkpoint inhibitors have improved clinical outcomes associated with numerous cancers, but high-grade, immune-related adverse events can occur, particularly with combination immunotherapy. We report the cases of two patients with melanoma in whom fatal myocarditis developed after treatment with ipilimumab and nivolumab. In both patients, there was development of myositis with rhabdomyolysis, early progressive and refractory cardiac electrical instability, and myocarditis with a robust presence of T-cell and macrophage infiltrates. Selective clonal T-cell populations infiltrating the myocardium were identical to those present in tumors and skeletal muscle. Pharmacovigilance studies show that myocarditis occurred in 0.27% of patients treated with a combination of ipilimumab and nivolumab, which suggests that our patients were having a rare, potentially fatal, T-cell-driven drug reaction. (Funded by Vanderbilt-Ingram Cancer Center Ambassadors and others.).
Conflict of interest statement
No other authors reported conflicts of interest.
Figures
Comment in
-
Myocarditis with Immune Checkpoint Blockade.N Engl J Med. 2017 Jan 19;376(3):292. doi: 10.1056/NEJMc1615251. N Engl J Med. 2017. PMID: 28099832 No abstract available.
-
Myocarditis with Immune Checkpoint Blockade.N Engl J Med. 2017 Jan 19;376(3):291-292. doi: 10.1056/NEJMc1615251. N Engl J Med. 2017. PMID: 28099833 No abstract available.
-
Myocarditis with Immune Checkpoint Blockade.N Engl J Med. 2017 Jan 19;376(3):290-1. doi: 10.1056/NEJMc1615251. N Engl J Med. 2017. PMID: 28102662 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- U01 HL098147/HL/NHLBI NIH HHS/United States
- K12 CA090625/CA/NCI NIH HHS/United States
- K08 HL119355/HL/NHLBI NIH HHS/United States
- U01 HL098153/HL/NHLBI NIH HHS/United States
- P50 CA098131/CA/NCI NIH HHS/United States
- U01 HL098162/HL/NHLBI NIH HHS/United States
- P50 GM115305/GM/NIGMS NIH HHS/United States
- U01 HL098163/HL/NHLBI NIH HHS/United States
- K23 CA204726/CA/NCI NIH HHS/United States
- R00 CA181491/CA/NCI NIH HHS/United States
- U01 HL098123/HL/NHLBI NIH HHS/United States
- HHMI/Howard Hughes Medical Institute/United States
- U01 HL098188/HL/NHLBI NIH HHS/United States
- R01 HL121363/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical