

Sepsis-3 definitions predict ICU mortality in a low-middle-income country
- PMID: 27807819
- PMCID: PMC5093106
- DOI: 10.1186/s13613-016-0204-y
Sepsis-3 definitions predict ICU mortality in a low-middle-income country
Abstract
Background: Sepsis-3 definitions were published recently and validated only in high-income countries. The aim of this study was to assess the new criteria's accuracy in stratifying mortality as compared to its predecessor (Sepsis-2) in a Brazilian public intensive care unit (ICU) and to investigate whether the addition of lactate values would improve stratification.
Methods: Retrospective cohort study conducted between 2010 and 2015 in a public university's 19-bed ICU. Data from patients admitted to the ICU with sepsis were retrieved from a prospectively collected database. ICU mortality was compared across categories of both Sepsis-2 definitions (sepsis, severe sepsis and septic shock) and Sepsis-3 definitions (infection, sepsis and septic shock). Area under the receiving operator characteristic curves were constructed, and the net reclassification index and integrated discrimination index for the addition of lactate as a categorical variable to each stratum of definition were evaluated.
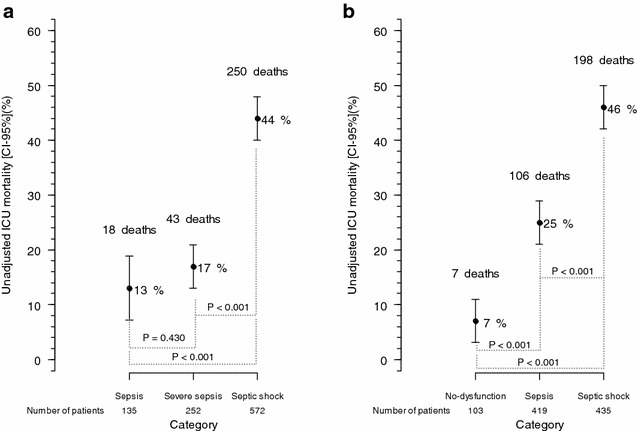
Results: The medical records of 957 patients were retrieved from a prospectively collected database. Mean age was 52 ± 19 years, median SAPS 3 was 65 [50,79], respiratory tract infection was the most common cause (42%, 402 patients), and 311 (32%) patients died in ICU. The ICU mortality rate was progressively higher across categories of sepsis as defined by the Sepsis-3 consensus: infection with no organ dysfunction-7/103 (7%); sepsis-106/419 (25%); and septic shock-198/435 (46%) (P < 0.001). For Sepsis-2 definitions, ICU mortality was different only across the categories of severe sepsis [43/252-(17%)] and septic shock [250/572-(44%)] (P < 0.001); sepsis had a mortality of 18/135-(13%) (P = 0.430 vs. severe sepsis). When combined with lactate, the definitions' accuracy in stratifying ICU mortality only improved with lactate levels above 4 mmol/L. This improvement occurred in the severe sepsis and septic shock groups (Sepsis-2) and the no-dysfunction and septic shock groups (Sepsis-3). Multivariate analysis demonstrated similar findings.
Conclusions: In a Brazilian ICU, the new Sepsis-3 definitions were accurate in stratifying mortality and were superior to the previous definitions. We also observed that the new definitions' accuracy improved progressively with severity. Serum lactate improved accuracy for values higher than 4 mmol/L in the no-dysfunction and septic shock groups.
Keywords: Infection; Intensive care unit; Lactate; Organ dysfunction; Sepsis; Septic shock.
Figures
References
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644–1655. doi: 10.1378/chest.101.6.1644. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
