

Clinical Outcome and Biological Predictors of Relapse After Nephrectomy Only for Very Low-risk Wilms Tumor: A Report From Children's Oncology Group AREN0532
- PMID: 27811504
- PMCID: PMC5145762
- DOI: 10.1097/SLA.0000000000001716
Clinical Outcome and Biological Predictors of Relapse After Nephrectomy Only for Very Low-risk Wilms Tumor: A Report From Children's Oncology Group AREN0532
Abstract
Objective: To determine if observation alone after nephrectomy in very low-risk Wilms tumor (defined as stage I favorable histology Wilms tumors with nephrectomy weight <550g and age at diagnosis <2 years) results in satisfactory event-free survival and overall survival, and to correlate relapse with biomarkers.
Patients and methods: The AREN0532 study enrolled patients with very low-risk Wilms tumor confirmed by central review of pathology, diagnostic imaging, and surgical reports. After nephrectomy, patients were followed without adjuvant chemotherapy. Evaluable tumors were analyzed for WT1mutation, 1p and 16q copy loss, 1q copy gain, and 11p15 imprinting. The study was powered to detect a reduction in 4-year EFS from 87% to 75% and overall survival from 95% to 88%.
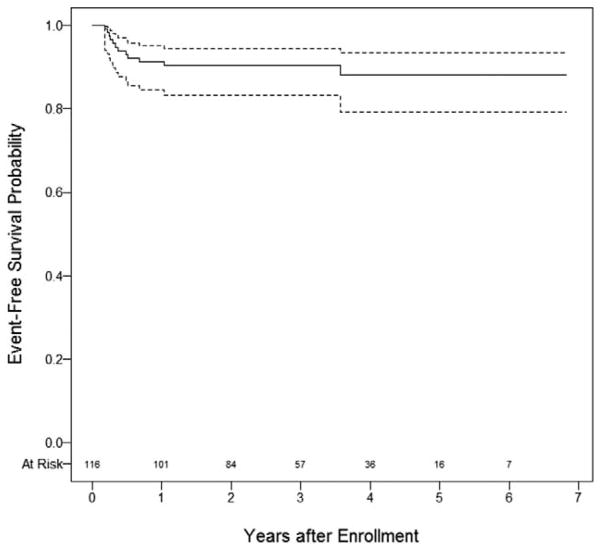
Results: A total of 116 eligible patients enrolled with a median follow up of 80 months (range: 5-97 months). Twelve patients relapsed. Estimated 4-year event-free survival was 89.7% (95% confidence interval 84.1-95.2%) and overall survival was 100%. First sites of relapse were lung (n = 5), tumor bed (n = 4), and abdomen (n = 2), with one metachronous tumor in the contralateral kidney (n = 1) at a median time of 4.3 months for those who relapsed (range 2.3-44 months). The presence of intralobar (P = 0.46) or perilobar rests (P = 1.0) were not associated with relapse (P = 0.16). 1q gain, 1p and 16q loss, and WT1 mutation status were not associated with relapse. 11p15 methylation status was associated relapse (20% relapse with loss of heterozygosity, 25% with loss of imprinting, and 3.3% relapse with retention of the normal imprinting (P = 0.011)).
Conclusions: Most patients meeting very low-risk criteria can be safely managed by nephrectomy alone with resultant reduced exposure to chemotherapy. Expansion of an observation alone strategy for low-risk Wilms tumor incorporating both clinical features and biomarkers should be considered.
Trial registration: ClinicalTrials.gov NCT00352534.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Cassady JR, Tefft M, Filler RM, et al. Considerations in the radiation therapy of Wilms’ tumor. Cancer. 1973;32:598–608. - PubMed
-
- Green DM, Jaffe N. The role of chemotherapy in the treatment of Wilms’ tumor. Cancer. 1979;44:52–57. - PubMed
-
- Green DM, Breslow NE, Beckwith JB, et al. Treatment with nephrectomy only for small, stage I/favorable histology Wilms’ tumor: a report from the National Wilms’ Tumor Study Group. J Clin Oncol. 2001;19:3719–3724. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
